Download
1 / 30
610 likes | 3.15k Views
Mammary Gland. Petek Korkusuz MD PhD. Learning Goals. To learn the development, histology and function of mammary glands. Development of Mammary Glands. Are a modified and highly specialized type of apocrine sweat glands.

E N D
Mammary Gland Petek Korkusuz MD PhD
Learning Goals • To learn the development, histology and function of mammary glands
Development of Mammary Glands • Are a modified and highly specialized type of apocrine sweat glands. • Consist of parenchyma, which is formed from ducts, and connective tissue stroma. • Parenchyma derives embryonically from surface ectoderm; stroma arises from surrounding mesenchyme. • Mammary buds begin to develop during the sixth week as solid downgrowths of the epidermis into the underlying mesenchyme • These changes occur in response to an inductive influence from the mesenchyme.
Development of Mammary Glands • Mammary buds develop as downgrowths from thickened mammary crests, which are thickened strips of ectoderm extending from the axillary to the inguinal regions • The mammary crests (ridges) appear during the fourth week but normally persist in humans only in the pectoral area, where the breasts develop • Each primary bud gives rise to several secondary mammary buds that develop into lactiferous ducts and their branches • Canalization of these buds is induced by placental sex hormones entering the fetal circulation. This process continues until late gestation, and by term, 15 to 19 lactiferous ducts are formed. • The fibrous connective tissue and fat of the mammary gland develop from the surrounding mesenchyme.
Development of Mammary Glands • A, Ventral view of an embryo of approximately 28 days showing the mammary crests. B, Similar view at 6 weeks showing the remains of these crests. C, Transverse section of a mammary crest at the site of a developing mammary gland. D to F, Similar sections showing successive stages of breast development between the 12th week and birth.
Development of Nipples and Areola • During the late fetal period, the epidermis at the site of origin of the mammary gland becomes depressed, forming a shallow mammary pit • The nipples are poorly formed and depressed in newborn infants. • Soon after birth, the nipplesusually rise from the mammary pits because of proliferation of the surrounding connective tissue of the areola, the circular area of skin around the nipple. • The smooth muscle fibers of the nipple and areola differentiate from surrounding mesenchymal cells.
Postnatal Development of Female Breast. • A, Newborn. B, Child. C, Early puberty. D, Late puberty. E, Young adult. F, Pregnant female. Note that the nipple is inverted at birth • (A). Normally the nipple elevates during childhood. Failure of this process to occur gives rise to an inverted nipple. At puberty (12-15 years), the breasts of females enlarge because of development of the mammary glands and the increased deposition of fat.
Postnatal Development • The rudimentary mammary glands of newborn males and females are identical and are often enlarged. • Some secretion, often called "witch's milk," may be produced caused by maternal hormones passing through the placental membrane into the fetal circulation. • Newborns breasts contain lactiferous ducts but no alveoli. Before puberty, there is little branching of the ducts. • In females, the breasts enlarge rapidly during puberty, mainly because of development of the mammary glands and the accumulation of the fibrous stroma and fat associated with them • . Full development occurs at approximately 19-20 years • The lactiferous ducts of male breasts remain rudimentary throughout life.
Gynecomastia • The rudimentary lactiferous ducts in males normally undergo no postnatal development. • Gynecomastia (Gr. gyne, woman + mastos, breast) refers to the development of the rudimentary lactiferous ducts in the male mammary tissue. • During midpuberty, approximately two thirds of boys develop varying degrees of hyperplasia of the breasts. This subareolar hyperplasia may persist for a few months to 2 years. • A decreased ratio of testosterone to estradiol is found • 80% of males with Klinefelter syndrome (XXY) have gynecomastia
Absence of Nipples (Athelia) or Breasts (Amastia) • Rare congenital anomalies may occur bilaterally or unilaterally. • Result from failure of development or disappearance of the mammary crests. • May also result from failure of mammary buds to form. • More common is hypoplasia of the breast, often found in association with gonadal agenesis and Turner syndrome
Aplasia of Breast • The breasts of a postpubertal female often differ in size. Marked differences are regarded as anomalies because both glands are exposed to the same hormones at puberty. • In these cases, there is often associated rudimentary development of muscles of the thoracic wall, usually the pectoralis major The thorax of an infant with congenital absence of the left pectoralis major muscle. Note the absence of the anterior axillary fold on the left and the low location of the left nipple. (From Behrman RE, Kliegman RM, Arvin AM [eds]: Nelson Textbook of Pediatrics, 15th ed. Philadelphia, WB Saunders, 1996.)
Supernumerary Breasts and Nipples • An extra breast (polymastia) or nipple (polythelia) occurs in approximately 1% of the female population as an inheritable condition. • An extra breast or nipple usually develops just inferior to the normal breast. • Supernumerary nipples are also relatively common in males; often they are mistaken for moles • Less commonly, supernumerary breasts or nipples appear in the axillary or abdominal regions of females developing from extra mammary buds that develop along the mammary crests. They become more obvious in women when pregnancy occurs. • Approximately one third of affected persons have two extra nipples or breasts. • Supernumerary mammary tissue very rarely occurs in a location other than along the course of the mammary crests. It probably develops from tissue that was displaced from these crests. A man and a female infant with extranipples (polythelia)
Inverted Nipples • Nipples fail to elevate above the skin surface after birth, remaining in their prenatal location (A) • May make breast-feeding of an infant difficult;
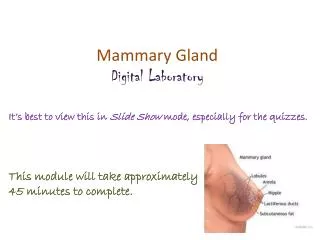
Mammary glands • Compound tubuloalveolar glands • Consist of 15 to 20 lobes radiating out from the nipple and are • Separated from each other by adipose and collagenous connective tissue. • Secrete milk, a fluid containing proteins, lipids, and lactose as well as lymphocytes and monocytes, antibodies, minerals, and fat-soluble vitamins • Provide the proper nourishment for the newborn.
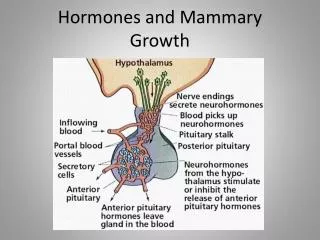
Mammary Glands Development • Develop in the same manner and are of the same structure in both sexes until puberty, • At puberty changes in the hormonal secretions in females cause further development and structural changes within the glands. • Secretions of estrogen and progesterone from the ovaries (and later from the placenta) and prolactinfrom the acidophils of the anterior pituitary gland initiate development of lobules and terminal ductules. • Full development of the ductal portion of the breast requires glucocorticoids and further activation by somatotropin.
Mammary Glands Development • Concomittant with these events is an increase in connective tissue and adipose tissue within the stroma, causing the gland to enlarge. • Full development occurs at about 20 years of age • Minor cyclic changes occur during each menstrual period, • Major changes occur during pregnancy and in lactation. • After age 40 or so, the secretory portions and some of the ducts and connective tissue elements of the breasts begin to atrophy, and they continue this process throughout menopause.
Gland Structure • The glands within the breasts are classified as compound tubuloalveolar glands, • Make 15 to 20 lobes radiating out from the nipple and separated from each other by adipose and collagenous connective tissue. • Each lobe is drained by its own lactiferous duct leading directly to the nipple, where it opens onto its surface. • Before reaching the nipple, each of the ducts is dilated to form a lactiferous sinus for milk storage and then narrows before passing through the nipple
Gland Structure • Near the opening at the nipple, lactiferous ducts are lined by a stratified squamous keratinized epithelium. • The lactiferous sinus and the lactiferous duct leading to it are lined by stratified cuboidal epithelium, • Smaller ducts leading to the lactiferous duct are lined by a simple columnar epithelium. • Stellate myoepithelial cells located between the epithelium and the basal lamina wrap around the developing alveoli and become functional during pregnancy
Body_ID: HC020037 Body_ID: quote515 Resting (Non secreting) Mammary Gland • Alveoli are not developed in nonpregnant women • nonpregnant women have the same basic architecture as the lactating (active) mammary gland, except that they are smaller and without developed alveoli, which occur only during pregnancy..
Lactating (Active) Mammary Glands • are activated by elevated surges of estrogen and progesterone during pregnancy to become lactating glands to provide milk for the newborn. • Terminal portions of the ducts branch and grow and the alveoli develop and mature • As pregnancy progresses, the breasts enlarge as a result of hypertrophy of the glandular parenchyma and engorgement with colostrum, • Colostrum is a protein-rich fluid, in preparation for the newborn. • Within a few days after birth, when estrogen and progesterone secretions have subsided, prolactin, secreted by acidophils of the anterior pituitary gland, activates the secretion of milk, which replaces the colostrum
Lactating (Active) Mammary Glands • During pregnancy, the terminal portions of the ducts branch and grow and develop secretory units known as alveoli. • Inset shows a longitudinal section of a gland and duct of the active mammary gland.
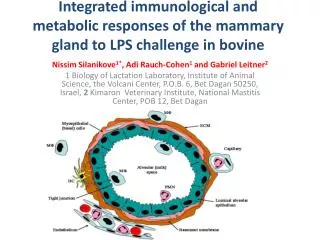
Alveoles and Alveolar Cells • The alveoliare composed of cuboidal cells partially surrounded by a meshwork of myoepithelial cells. • These secretory cells possess abundant RER and mitochondria, several Golgi complexes, many lipid droplets, and numerous vesicles containing caseins (milk proteins) and lactose. • Not all regions of the alveolus are in the same stage of production, because different acini display varying degrees of preparation for synthesis of milk substances Electron micrograph of an acinar cell
Milk Secretion from Alveolar Cells • The secretions of the alveolar cells are of two kinds: lipids and proteins. • Stored as droplets within the cytoplasm. • Released from the secretory cells by the apocrine modeof exocytosis, • Small droplets coalesce to form larger and larger droplets that move to the periphery of the cell. • Once there, they project as cytoplasmic blebs into the lumen; eventually, the lipid droplets containing blebs are pinched off and become part of the secretory product. • Each bleb consists of a central lipid droplet surrounded by a narrow rim of cytoplasm and enclosed by a plasmalemma. • Proteinssynthesized within these secretory cells are liberated from the cells by the merocrine mode of exocytosis in much the same manner as would be expected of other cells that synthesize and release proteins into the extracellular space
Areola and Nipple • The circular, heavily pigmented skin in the center of the breast is the areola. • Areola contains sweat glands and sebaceous glands at its margin as well as areolar glands (of Montgomery) that resemble both sweat and mammary glands. • In the center of the areola is the nipple, a protuberance covered by stratified squamous epithelium containing the terminal openings of the lactiferous ducts. • In fair-skinned individuals, a pinkish color is imparted to the nipple as a result of the color of blood in the rich vascular supply within the long dermal papillae that extend near its surface. • During pregnancy, the color becomes darker because of increased pigmentation of the areola and the nipple.
Areola and Nipple • The core of the nipple is composed of dense collagenous connective tissue with abundant elastic fibers connected to the surrounding skin or interlaced within the connective tissue and a rich component of smooth muscle cells. • The wrinkling of the skin on the nipple results from the attachments of the elastic fibers. • The abundant smooth muscle fibers are arranged in two ways: circularly around the nipple and radiating longitudinally along the long axis of the nipple. • The contraction of these muscle fibers is responsible for erection of the nipple. • Most of the sebaceous glands located around the lactiferous ducts open onto the surface or sides of the nipple, although some open into the lactiferous ducts just before those ducts open onto the surface.
Mammary Gland Secretion: Milk Production • Prolactin is responsible for the production of milk • Oxytocin is responsible for the milk ejection reflex. • Although the mammary gland is prepared to secrete milk even before birth, certain hormones prohibit this. • When the placenta is detached in the adult female, prolactin from the anterior pituitary stimulates the production of milk, which reaches full capacity in a few days. • Before that, for the first 2 or 3 days after birth, a protein-rich thick fluid called colostrum is secreted. • Colostrumis a high-protein secretion, rich in vitamin A, sodium, and chloride, also contains lymphocytes and monocytes, minerals, lactalbumin, and antibodies (immunoglobulin A) to provide nutrition and passive immunity to the newborn. • Milk, usually produced by the 4th day after parturition, is a fluid that contains minerals, electrolytes, carbohydrates (including lactose), immunoglobulins (mostly immunoglobulin A), proteins (including caseins), and lipids. • Production of milk results from the stimuli of sight, touch, handling of the newborn, and anticipation of nursing, events that create a surge in prolactin release.
Mammary Gland Secretion: Milk Production • Once initiated, milk production is continuous, with the milk being stored within the duct system. • Concomitant with the production of prolactin, oxytocin is released from the posterior lobe of the pituitary. • Oxytocin initiates the milk ejection reflex by inducing contractions of the myoepithelial cells around the alveoli and the ducts, thus expelling the milk. • Mothers who cannot breast-feed their infants on a regular feeding schedule are inclined to suffer from poor lactation. This may motivate a decision to discontinue nursing altogether, with the result that the infant is deprived of the passive immunity conferred by ingesting antibodies from the mother.
Breast cancer • Seen second to lung cancer as one of the major causes of cancer-related death in women, • may be of two different types: ductal carcinoma of the ductal cells and lobular carcinoma of the terminal ductules. • Detection must be early, or the prognosis is poor because the carcinoma may metastasize to the axillary lymph nodes and from there to the lungs, bone, and brain. • At the recommendation of the medical profession, early detection through self-examination and mammography has helped to reduce breast cancer mortality rates. • In 2005, approximately 270,000 women and 1700 men were diagnosed with breast cancer in the United States and approximately 40,000 women and 500 men died of breast cancer. • There is an inverse relationship between the age of the woman and her risk of contracting the disease, in that in 2005 1 out of 2200 women less than 30 years of age contracted breast cancer, whereas 1 out 54 and 1 out of 23 women less than 50 and 60 years of age, respectively, contracted breast cancer. • Although breast cancer is more likely to occur at an older age, younger women tend to have more aggressive breast cancers
Summary: Mammary Glands • Modified and highly specialized type of apocrine sweat glands • Consist of parenchyma, which is formed from ducts, and connective tissue stroma. • Parenchyma derives embryonically from surface ectoderm; stroma arises from surrounding mesenchyme (inductive interactions). • The 6-week embryo has two ventral ridge-like thickenings of epidermis, the mammary (milk) lines, extending from axillae to the inguinal area. • The major part of each ridge disappears almost immediately, but one pair remains in the pectoral area and penetrates the mesenchyme. • Then, 15-25 solid epithelial cords develop from each and are later canalized to form future lactiferous ducts. • Mesenchyme gives rise to loose connective tissue around each duct. Denser connective tissue forms septa between them to divide the gland into lobes. • Childhood gland structure is rudimentary and alike in both sexes. • At puberty, glands in girls grow and undergo structural changes directly influenced by ovarian hormones (estrogen and progesterone). • They are not fully formed and functional, however, until pregnancy and lactation. • In pregnancy, terminal ends of ducts develop into hollow, sac-like secretory alveoli, which are lined by simple cuboidal epithelium. • Women who give birth have highly specialized exocrine glands that synthesize and secrete milk. Prolactin, human placental lactogen, estrogen, and progesterone in the presence of prolactin from the anterior pituitary result in milk production; oxytocin from the posterior pituitary induces milk release.