Download
1 / 38
500 likes | 2.16k Views
Swallowing Difficulties (Dysphagia). Clare Linger & Francesca Jenkins Speech and Language Therapists. Agenda. The normal swallow process Who has dysphagia? What can go wrong? Signs and symptoms of dysphagia Practical session – experimental feeding How to manage dysphagia Oral hygiene

E N D
Swallowing Difficulties (Dysphagia) Clare Linger & Francesca Jenkins Speech and Language Therapists
Agenda • The normal swallow process • Who has dysphagia? • What can go wrong? • Signs and symptoms of dysphagia • Practical session – experimental feeding • How to manage dysphagia • Oral hygiene • Modified diet and fluids • Practical session – modifying fluids / categorising diet • Role of MDT and SALT in managing swallowing difficulties • Summary
Aims & Objectives • To recap understanding of the normal swallowing process. • To understand the SLT and MDT role in dysphagia. • To identify overt signs of aspiration and recognise patients on the ward who show swallowing difficulties. • To have knowledge of modified diets/fluids and understand importance of different consistencies. • To be aware of how to assist with feeding, optimising swallow safety.
Dysphagia and Stroke • Approximately 45% of patients admitted to hospital with a CVA have dysphagia. (Royal College of Physicians 2004) • Numerous studies have investigated site of lesion and dysphagia in CVA. Lack of association between site of lesion and aspiration, larger vessel infarcts show higher occurrence of aspiration and older subjects with larger CVAs aspirate more. (Singh & Hamdy 2006)
NICE Quality Standards for Stroke 2010 • Patients with acute stroke have their swallowing screened by a specially trained healthcare professional within 4 hours of admission to hospital, before being given any oral food, fluid or medication, and they have an ongoing management plan for the provision of adequate nutrition. • If the admission screen indicates problems with swallowing, the person should have a specialist assessment of swallowing, preferably within 24 hours of admission and not more than 72 hours afterwards. • Patients with stroke are assessed and managed by stroke nursing staff and at least one member of the specialist rehabilitation team within 24 hours of admission to hospital, and by all relevant members of the specialist rehabilitation team within 72 hours, with documented multidisciplinary goals agreed within 5 days. • People with suspected aspiration on specialist assessment or who require tube feeding or dietary modification for three days should be: • reassessed and considered for instrumental examination • referred for dietary advice
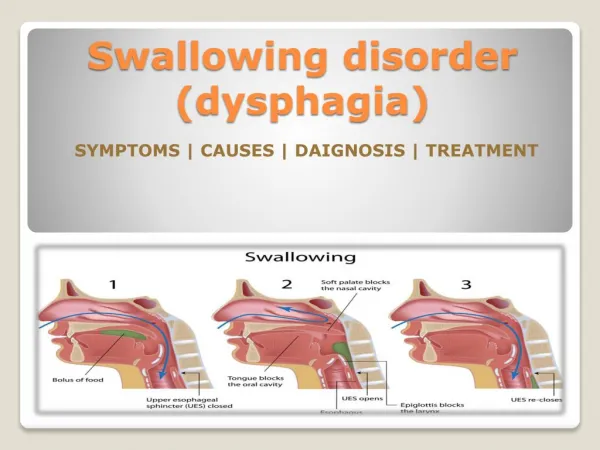
The Normal Swallow • A complex co-ordination of a number of muscles and nerves. • 5 Stages – • Anticipatory Phase • Oral Preparatory Phase • Oral Phase • Pharyngeal Phase • Oesophageal Phase
Lip Hard palate Anatomical Structures
Neurology of Swallowing • Involves 7 cranial nerves and ~ 30 muscles • CN I –Olfactory • Contains sensory fibres for smell • CN V -- Trigeminal • contains both sensory and motor fibres that innervate the face • important in chewing • CN VII -- Facial • contains both sensory and motor fibres • important for sensation of oropharynx & taste to anterior 2/3 of tongue • CN IX -- Glossopharyngeal • contains both sensory and motor fibres • important for taste to posterior tongue, sensory and motor functions of the pharynx • CN X -- Vagus • contains both sensory and motor fibres • important for taste to oropharynx, and sensation and motor function to larynx and laryngopharynx. • important for airway protection • CN XI – Accessory • Contains primarily motor fibres • Important for movement of head and shoulders • Important for muscles of the larynx • CN XII -- Hypoglossal • contains motor fibres that primarily innervate the tongue
Anticipatory Phase • Environmental factors • People involved and their communication and manner • Presentation of food • Any assistance required e.g. hand-over-hand feeding • Cognitive aspects e.g. -Attention to the food - Any neglect - Sensory problems • CN I
Oral Preparatory Phase • Get food ready to swallow • Lips close • Solid food chewed & mixed with saliva • Tongue gathers food into bolus • Airway open • CN V, VII,, XI, XII
Oral Phase(voluntary stage - 1 sec) • Tongue moves bolus back towards pharynx • Soft palate raised • When bolus reaches faucal arches swallow reflex is triggered • CN V, IX, X
Pharyngeal Phase(automatic stage < 1 sec) • Elevation and retraction of soft palate • Retraction of base of tongue • Elevation and forward movement of larynx • Closure of larynx by epiglottis & adduction of vocal folds • The swallow is triggered during this stage • CN IX, X, XI, XII
Oesophageal Phase • Patient may report food gets “stuck” • More difficulty with food than fluids • A gastroenterologist and dietician are the most appropriate port of call. • Currently SLT is not involved with oesophageal phase dysphagia
DEFINITION OF DYSPHAGIA • ‘The term dysphagia is used to describe eating and drinking disorders which may occur in the oral, pharyngeal and oesophageal stages of the swallow.’ RCSLT (2006)
Populations who present with Dysphagia • CVA / TIA • Dementia • Progressive diseases such as; PD / MS / MND • HI • Head and Neck Cancer • ALD • Old Age • Other
Pre-Oral & Oral Stage Weak/uncoordination of upper limb muscles Difficulty getting food/drink to mouth Weak facial muscles Food/drink leaking from the mouth Excess saliva Drooling Weak/uncoordinated oral movements Oral residue – food/fluid collecting in the cheeks/on tongue Swallowing Difficulties
Swallowing Difficulties • Pharyngeal Stage • Delayed swallow - Risk of aspiration pre-swallow • Reduced airway protection - Risk of aspiration during swallow • Reduced elevation of larynx - Residue at the top of the airway • Weak throat muscles - Residue throughout the pharynx • Sticking sensation in throat • Weak/uncoordinated movements of throat muscles - Risk of aspiration post-swallow • Aspiration/penetration - Food/fluid entering the airway • Oesophageal stage • Reflux – Risk of aspiration and discomfort
Factors which influence swallowing: • Level of alertness • Positioning • Appetite • Taste • Presentation of food • Cognition (distractibility, impulsivity etc.) • Chest status • Sensory loss • Oral hygiene • Dentures • Sitaphobia (dislike of eating in company) • Depression
Possible consequence of dysphagia • Airway penetration • Entry of bolus into the laryngeal vestibule but not below the level of the vocal cords • Aspiration • entry of bolus into the airway below the level of the true vocal cords • Silent Aspiration • no immediate cough, change in vocal quality or overt clinical signs of aspiration
Practical 1 -EXPERIMENTAL FEEDING • Pastille with poor tongue movement • Liquid with reduced lip seal • Eating/drinking with poor posture (e.g. slumped to one side or laid back) • Being fed by partner who is standing over you and not communicating when the next mouthful is coming
MAKING IT EASIER AND SAFER TO EAT & DRINK • Level of alertness • Being aware of an individual’s ability to stay alert • Oral Hygiene • What is mouth care? • Who is it suitable for? • Why is it important? • Posture • Sitting upright/ Supported if necessary • Head flexed • Environment • Reduce distractions • Social occasion • Plenty of time • Food/drink modification as recommended
Oral Hygiene • Aspiration of oral secretions and their bacteria is increasingly being recognized as an important factor in pneumonia (H Sasaki et al 2002, Langmore et al 1998) • A number of studies have shown that the mouth canbe colonized by respiratory pathogens and serve as a reservoirfor these organisms. • Other studies have demonstrated that oralinterventions aimed at controlling or reducing oral biofilmscan reduce the risk of pneumonia in high-risk populations. (Scannapieco 2006) • Takentogether, the evidence is substantial that improved oral hygienemay prevent pneumonia in vulnerable patients.
Oral Hygiene • To ensure clean healthy mouth • Must do regularly – ideally 1-2 hourly • Use squeezed out oral sponges, swabs or child’s toothbrush with small amount of toothpaste • Ensure when using toothpaste that the patient tips their head forwards to prevent aspiration • To moisten lips, tongue, gum, palate • Remove thick or crusted saliva
Nutritional aspects of management: In order to maintain adequate nutrition the following may be appropriate: • Alternative feeding (NG/PEG) • Alternative feeding as an adjunct to oral trials • Supplements to support oral intake (such as ensures)
Modifying Fluids & Diet • Why do we make these recommendations? • To aim to make swallowing as easy, safe and efficient as possible. • To continue oral intake for as long as possible.
Fluid & Diet consistencies • Thin fluids – no thickener • Syrup Thick fluids (2 scoops per 200ml) • Runny Custard Thick fluids (3 scoops per 200ml) • Pudding Thick fluids (4 scoops per 200ml) • N.B. Above measurements are for Thick & Easy – different measurements are needed for different thickening agents • Puree (Puree B and Puree C where available) • Soft • Normal
DRINK CONSISTENCY Hot and cold drinks (standard size cup) • Syrup:leaves thin coat on back of spoon can drink through straw • Custard:leaves thick coat on back of spoon cannot drink through straw • Pudding:needs to be taken with spoon cannot drink from cup or straw • Pre-thickened drinks
Practical 2 -Thickening Exercise • Following the instructions handed out, thicken three cups of water to each of the following consistencies: • Syrup thickened fluids • Runny Custard Thickened fluids • Pudding thickened fluids • Each member of the group to sample thickened fluids.
Difficult Foods Mixed consistencies Medication Cornflakes Minestrone soup Skins Sausages Tomatoes Sweetcorn Fibrous foods Pineapple Lettuce Red Meats Dry Crumbly foods Biscuits Crisps Nuts Cake
Activity: Sort the lists of food into groups White fish in crispy batter Yoghurt Egg mayonnaise sandwich (no crusts) Peanuts Creamy smooth mashed potato Chilli con carne with rice Macaroni cheese Digestive biscuit Thick custard Shepherds pie Smooth porridge Poached white fish
Role of MDT in Managing Swallowing Difficulties • Identify patients at risk • Those who have a diagnosis that may cause swallowing difficulties • Monitor patients for signs of aspiration • Refer appropriate patients to Speech and Language Therapy service • Ensuring good oral hygiene • Give correct consistency fluids and diet in best possible way • Ensuring safe swallow strategies
SLT Role in Dysphagia • Oromotor examination • Complete assessment of oral preparatory, oral and pharyngeal stages of the swallow • Trials of strategies to improve swallow safety • Assessment with modified diet and/or fluids • Exercises to improve range, rate and strength of specific muscle movement
SLT Role cont… • Review as appropriate • Liaison with family/carers, physiotherapy, occupational therapy, dietetics, nutrition team, nursing staff, health care assistants and the medical team • May consider videofluoroscopy • Liaison with medical team, patient, family/carers regarding alternative feeding • Training nursing and medical staff
Summary • The normal swallow process • Patients who may have dysphagia • Signs and symptoms of dysphagia • Signs of aspiration • Role of SALT • Role of MDT • Food and fluid consistencies