Download
1 / 21
380 likes | 1.67k Views
Eye movement disorder. Dr Kayed CNS Module- week 4. Extraocular muscle. All Extraocular muscles are supplied by oculomotor nerve except superior oblique by the trochlear nerver and lateral rectus by abducent nerve (SO)4 [(LR)6 ]3. Extraocular muscles function. Testing extraocular muscles.

E N D
Eye movement disorder Dr Kayed CNS Module- week 4
Extraocular muscle All Extraocular muscles are supplied by oculomotor nerve except superior oblique by the trochlear nerver and lateral rectus by abducent nerve (SO)4 [(LR)6 ]3
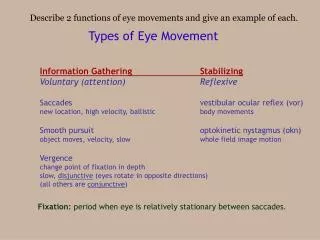
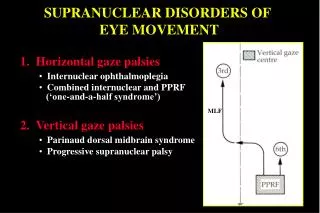
Gaze Centers • The direction of the movement is determined by which eye muscles are activated. Although in principle any given direction of movement could be specified by independently adjusting the activity of individual eye muscles, the complexity of the task would be overwhelming. Instead, the direction of eye movement is controlled by the local circuit neurons in two gaze centers • Vertical gaze centers are in the midbrain reticular formation. • Horizontal gaze center is in Paramedian pontine reticular formation (PPRF) in the pons • The gaze centers are controlled by vestibular nucleus, , frontal eye field and superior colliculus
Normal horizontal movements of the eyes to the right: Activation of the right horizontal gaze center (the PPRF) by the frontal eye field leads to increased activity of the right abducent nucleus. The lower motor neurons innervate the lateral rectus muscle of the right eye. The internuclear neurons innervate lower motor neurons in the contralateral oculomotor nucleus, which in turn innervate the medial rectus muscle of the left eye.
Gaze centers lesions • An acute lesion of the right frontal eye field will interrupt the horizontal gaze pathway and the eyes will be moved toward the side of the lesion by the unopposed lesion of the opposite frontal eye field.
A unilateral lesion in the pons at the level of the PPRF on the left will paralyze leftward eye movements
Evaluating eye movement in unconscious patient: Oculocephalic Reflex (Doll's Eyes)
Evaluating eye movement in unconscious patient: Oculovestibular reflex • Reflex triggered by stimulation of the labyrinth upon injection of cold water into the external auditory canal, and that leads to a nystagmus with a rapid phase to the side of the stimulated ear.
Terminology related to eye movement disorders • Exotropia: eye deviated outward • Esotropia: eye deviated inward • Exophthalmos: eye bulging outward • Enophthalmos: relative recession (backward or downward displacement) of the eye into the bony orbit. • Ptosis: dropping of the eyelid • Miosis: constriction of the pupils • Mydriasis: dilitation of the pupils
Exotropia Esotropia Exophthalmos ptosis Miosis Enophthalmos Mydriasis
Opthalmoplegia • Ophthalmoplegia is a paralysis or weakness of one or more of the muscles that control eye movement. The condition can be caused by any of several neurologic disorders: • Miller- fisher variant of Guillain Barre Syndrome (MFV-GBS): GBS is acute inflammatory demylination neuropathy. MFV-GBS the patient will present with areflexia, ataxia, and opthalmoplegia • Thiamine Deficiency • Wernicke's encephalopathy: in alcoholic with thiamine deficiency they will present with encephalopathy, opthalmoplegia and ataxia • Opthalmoplegic Migraine
Oculomotor (III) Cranial Nerve palsy • Typical presentation: • Ptosis (dropping of eyelid) • Mydriasis (dilatation of pupil) • Eye deviated outward and downward • Absent pupillary reflex: eye is not reactive to light • III cranial nerve palsy is classified into • Pupillary sparing : in microvascular diseases (suggesting diabetes) • Non- pupillary sparing (complete Oculomotor nerve palsy) mainly caused by aneurysm or herniation
Complete III cranial nerve palsy: Ptosis, mydriasis, & external rotation is most consistent with structural pathology.
Abducent palsy • Eye deviated medially • It could be unilateral which suggests diabetes • Or bilateral: may result from increased intracranial pressure or benign intracerebral hypertension
Internuclear ophthalmoplegia • Defect of oculomotion characterized by a disconjugate gaze, in which the eyes move independently on attempted lateral gaze. It is due to a pontine lesion with damage to the medial longitudinal fasciculus which links the eyes together. • The main causes of internuclear ophthalmoplegia are multiple sclerosis, pontine infarction or haemorrhage and infiltrating tumours of the brain stem.
Nystagmus • Nystagmus is an involuntary rhythmic shaking or wobbling of the eyes. • It can occur normally, such as when tracking a visual pattern. or may also be abnormal, usually in situations where one would want the eyes to be still, but they are in motion.
Other caused of eye movement disorders • In any patient with Extraoculor muscle disorder we should think of • Myasthenia Gravis • Thyroid ophthalmopathy • Pseudo Internuclear ophthalmoplegia