Download
1 / 24
240 likes | 262 Views
Explore the challenges in identifying deteriorating patients and learn actionable steps to improve their safety. This report delves into communication, management, monitoring systems, and error wisdom to enhance patient care. Recommendations include establishing a 'Deterioration Recognition Group' and integrating patient safety into daily healthcare practices.

E N D
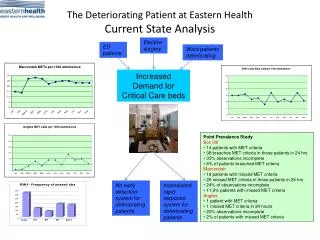
Why are deteriorating patients not recognised or not acted upon and what can we do about it? Kate Beaumont Strategy Advisor NPSA
‘The top priority, top priority is always safety’ ‘It doesn’t cost a fortune to have patient safety’ Secretary of State for Health – Alan Johnson. House of Commons 15th October 2007
The top priority but why is it so difficult to recognise and respond appropriately to deterioration?
Launch of NPSA Report Recognising and responding appropriately to early signs of deterioration in hospitalised patients 16 November 2007
Method – triangulation • Focus groups with doctors and nurses • Semi-structured interviews with clinicians • Aggregate Root Cause Analysis • Ethnographic analysis (observational study and interviews) • Literature review to seek to answer why
NPSA contributory factors classification • Communication factors • Working conditions and environmental factors • Task factors • Education and training factors • Patient factors • Team and social factors • Organisational factors • Equipment and resources factors • Individual factors
Management and workload – the issues • prioritising competing demands • value of doing observations sometimes not well understood • lack of strong and experienced ward leadership From the report, Appendix 1 Checklist
Are you encouraging colleagues to see observations as an important element of their work? “When staff come on duty, they’ve got several must-dos. Patients must get their breakfast, drugs have to be given out and staff have to prepare for 10 o’clock hospital discharges. This is also the time to start ward rounds. There’s a lot of pressure in the early part of morning. So when do you fit in doing your obs?” seniornurse
Do you have a suitably experienced ward leader on every shift who maintains an overview of the wellbeing of all patients? “For some of the experienced nurses, you often hear people talk about the 'gut feeling'… you observe, you look closer, you question your patients. Somewhere along the line something will give information that a younger member of staff could overlook” senior nurse
Communication and teamwork – the issues • being able to communicate information succinctly and to make requests assertively • good working relationships needed for effective communication • both nurses and doctors reluctant to seek more senior help if they do not get the support they need from their first level contact
Do you think communication can be improved in relation to deteriorating patients? Have you considered introducing a communication tool such as SBAR or RSVP? “Sometimes they call you and ask, ‘What do you want us to do?’ and you’ve written it in the notes.” junior doctor “Doctors assume that if it’s in the medical notes nurses will read it. But if they’re busy doing something this is not going to be case.” senior nurse
Monitoring and escalation procedures – the issues • routine observations frequently carried out by healthcare assistants or student nurses • Staff often did not have sufficient training to understand the relevance of any findings and how to communicate these onwards effectively and promptly
Are you using physiological track and trigger systems to monitor all patients? Have you considered introducing colour-coded observation charts? “A nurse may not pick up the signs because of a lack of training or understanding. Or they might not be seeing it, they’re writing it down and not seeing what’s in front of them.”staff nurse
James Reason uses the Western Mining Corporation in Western Australia as an exemplar of error wisdom, their motto is – ‘Take time, take charge’
Being error wise • Accept errors can and will occur • Assess the local constraints before embarking on a task • Have contingencies ready to deal with anticipated problems • Be prepared to seek more qualified assistance • Overcome professional courtesy and check colleagues’ knowledge and expertise • Appreciate that the path to incidents is paved with false assumptions
Conclusions and recommendations of the report Every acute trust should establish - a‘Deterioration Recognition Group’which leads and coordinates efforts to improve the safety of patients who are vulnerable to unexpected deterioration.
TheDeterioration Recognition Groupcan learn from other trusts (their local equivalents) – resources, good practice examples and contact details are provided in the report TheDeterioration Recognition Groupcan use the checklist of reflective questions within the report to identify effective implementation strategies sensitive to local organisation, culture and present policies.
National Patient Safety Campaign Making patient safety part of everyday healthcare: a new national campaign to encourage people and organisations in the NHS to make patient safety part of everything they do
Deterioration The goal • To reduce in-hospital cardiac arrest and mortality rate through earlier recognition and treatment of the deteriorating patient. • This intervention addresses six key areas relating to deterioration: • Physiological observations should be recorded for all adult patients in acute hospital settings. • Physiological observations should be recorded and acted upon by staff who have been trained to undertake these procedures and understand their clinical relevance. • Physiological track and trigger systems should be used. • There should be a graded response strategy. • An escalation protocol should be in place. • A communication tool should be used.
“The five most dangerous words in health care are; "it could never happen here.”Professor Sir Liam Donaldson
Active failures are like mosquitoes. They can be swatted one by one, but they still keep coming. The best remedies are to create more effective defences and to drain the swamps in which they breed. The swamps, in this case, are the ever present latent conditions. James Reason
Acknowledgements • NHS nursing and medical staff who shared their experiences in the interviews and focus groups • NHS risk managers who shared anonymised root cause analysis reports • Researchers who conducted the studies for this report: Mary Dixon-Woods, Anu Suokas and Richard Lilford (Ethnographic analysis), Claire Blackett and Steve Cross (Aggregate Root Cause Analysis), Kristina Staley and Judy Wilson (Interviews with Clinicians), Kate Beaumont, Dagmar Luettel, Jane Carthey, Joanne Hillier, Alison Hugget, Louise Thomas (Focus groups) and Mig Muller (Literature review) • Leroy Edozien, Jenny Firth-Cozens, Saxon Ridley, Charles Vincent, Patricia Young and Suzette Woodward who helped to explore the contributory factors
Further information can be found at: www.npsa.nhs.uk 4 - 8 Maple Street, London, W1T 5HD or email: Catherine.beaumont@npsa.nhs.uk