Download
1 / 14
140 likes | 537 Views
High Performance Computing in Surgical Simulation. An Approach Using Compact Support Radial Basis Functions. Mark Wachowiak, Xiaogang Wang, Aaron Fenster, Terry Peters Imaging Research Laboratories Robarts Research Institute London, ON N6A 5K8. Surgical simulation for:

E N D
High Performance Computing in Surgical Simulation. An Approach Using Compact Support Radial Basis Functions Mark Wachowiak, Xiaogang Wang, Aaron Fenster, Terry Peters Imaging Research Laboratories Robarts Research Institute London, ON N6A 5K8
Surgical simulation for: Pre-operative planning Training Developing new procedures Basic biomedical research Tissue properties Response to therapy Soft Tissue Modeling and Surgical Simulation One of the goals of surgical simulation is to facilitate planning of minimally invasive procedures and to transfer the results to the operating room. Simulation, like robotics and tracking systems (shown above), provides great benefits to minimally invasive surgery. Biomechanical properties are incorporated into surface and volumetric models generated from real patients’ data/images. The resulting physical model can then be used in pre-procedural planning or for simulation for surgical training.
Geometric models Advantages Fast computation time real time performance can be obtained. Relatively easy to implement. Visually compelling. Disadvantages Do not take physical properties into account. May be very inaccurate for complex tissue. Haptic feedback is “empirical”. Examples Free-form deformation. Chain-mail. Sphere-filled models. Physical models Advantages Very realistic. Can be used to study tissue behaviour . Haptic feedback computations are straightforward. Disadvantages Very slow. Much pre-processing is required Relatively difficult to implement. May also be inaccurate for large topology changes (cutting, suturing). Examples Finite elements (widely-accepted “gold standard”). Mass-spring models (a little better speed). Hybrid geometric-physical approaches. Soft Tissue Modeling Approaches
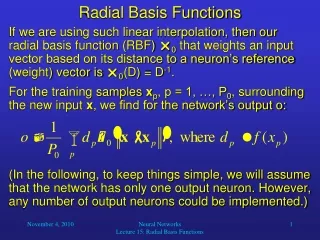
Radial Basis Functions (RBFs) Compact Support Radial Basis Functions (CSRBFs) • A class of basis functions that can be used to model soft tissue deformations. • Thin plate splines are also widely used for this purpose • Many such functions exist, including multiquadratics and Gaussian functions. • Can provide visual realism in surgical simulation, but often requires parameters to model biomechanical properties. • RBF methods have an inherentparallelism. • Very often have an undesirable global effect – the whole tissue deforms when only a small local area is perturbed. • Proposed by H. Wendland in 1995 • Unlike other RBFs or spline functions, CSRBFs have a local effect. • Locality is controlled by a user-specified parameter. • CSRBF matrices are positive definite, and are therefore guaranteed to be invertible. • CSRBF matrices are also often sparse, and can be inverted with specialized methods. • Unlike other RBF and spline functions, no polynomial terms are required.
Examples of CSRBFs Quadratic 4th order 6th order Logarithmic/4th order r > 0 otherwise Plots of CSRBFs
Landmarks Placed on (virtual) surgical instruments, and on the (virtual) surface and in the interior of tissue. Collision detection of the tissue surface and surgical instrument select source landmarks. As the instrument deforms the tissue, the source landmarks (from collision detection) move toward the new target landmarks on the surgical tool, causing a deformation. Tissue properties: Stiffness: modeled by locality parameter (a). Elasticity (shape of deformation): modeled with smoothness of CSRBF. Internal tissue landmarks also help to simulate stiffness. CSRBFs in Soft Tissue Modeling applied force surface Stiffness is modeled by the locality parameter (width of deformation) and by internal landmarks. Elasticity is modeled by shape of RBF function.
Example 2D deformation with 4 control points and 10 internal landmarks Colors indicate the density, measured in terms of surface area of the “material” after deformation. Red values indicate higher compression, corresponding to higher density after deformation. y2, a = 8 y6, a = 8 y2, a = 12 y6, a = 12
Example 2D deformation with 4 control points and 10 internal landmarks Colors indicate the density, measured in terms of surface area of the “material” after deformation. Red values indicate higher compression, corresponding to higher density after deformation. y2, a = 20 y6, a = 20 y2, a = 40 y6, a = 40
Tissue Deformation Experiments • The efficacy of this deformation model is demonstrated on data from a 3D prostate image for the application of needle insertion for implanting radioactive seeds for brachytherapy. • This procedure is minimally invasive. A critical factor in the success of this procedure is accurate seed delivery based on a dosimetric plan that maximizes destruction of the cancerous cells, while minimizing damaging to healthy tissue. • The online simulation involves: • Interactive visual simulation (30Hz) • Haptic feedback (1 KHz) • TCP/IP-based communication. • Soft tissue model • Volumetric prostate generated from a pre-operative 3D ultrasound volume and its segmented boundary. • 8 internal landmarks. • 14,560 3D points, including 1,200 on the surface. • A simple collision detection algorithm was used to identify the landmark corresponding to the contact point between the needle tip. • Timing experiments were run on a 4-CPU shared-memory 1.0GHz HP/ Compaq® ES45 system. • The following timing experiments were performed: • Four (4) CSRBF functions • From 1 to 41 landmarks • Three support sizes: • a = 1 (sparse matrix) • a = 10 • a = 20 (dense matrix) • All timing experiments were performed on the prostate data, as described above. • 100 trials were performed for each experiment. Mean values are reported. • The interpolation over all 3D points was parallelized. • Parallelization was performed with OpenMP.
Timing Results y2, a = 10 y4, a = 10 ylog, a = 10 1 CPU 1 CPU 1 CPU 4 CPUs 4 CPUs 4 CPUs y2, 1 and 4 CPUs y4, 1 and 4 CPUs ylog, 1 and 4 CPUs
Deformation Results Target for seed placement Mesh representations y4, a = 6 (local) Mesh representations y4, a = 12 With the large locality parameter (a = 24), the deformation effect was more global, and the entire prostate base was pushed inward. Mesh and surface representations y6, a = 24 (global)
Discussion • The prostate deformations were visually realistic, with the shape controlled by the locality parameter and CSRBF selection. • The method scales well for all CSRBFs. • As expected, the least complex CSRBF (y2) had the highest time performance. The most complex CSRBF (ylog) was the most time-complex. The performance of y4 was marginally better performance than that of y6. • Using 4 CPUs, there is only a marginal difference between computation time for the sparse and dense matrices. • Small “glitches” in the computation times for all experiments for 12 and 32 landmarks is most likely due to caching effects on the specific architecture used.
Conclusions • For applications where real-time performance is required, compact support radial basis functions provide visually compelling deformations for soft tissue modeling. • These methods are also easily parallelized, and scale well on shared memory architectures. • Future work includes: • Parallelizing more of the simulation, including CSRBF function evaluation and sparse matrix inversion. • Applying RBFs and CSRBFs within a finite element framework, incorporating physical parameters. These techniques are known as mesh-free methods, and address many of the problems inherent in classical finite element approaches. • The methods must be tested on a wide variety of clinical data, including non-convex and non-homogeneous tissue. • Clinical validation is required.
Acknowledgements • The authors gratefully acknowledge Ravi Gupta, Jeff Gardiner, and Baolai Ge for technical and scientific support, Drs. Gerard Guiraudon, Renata Smolíková-Wachowiak,and Hualiang Zhong for helpful discussions, and the Virtual Cardiac Surgery Planning (VCSP) group at the Imaging Research Laboratories, Robarts Research Institute: Martin Wierzbicki, Guy-Anne Turgeon, Dr. Stan Szpala, and John Moore. • Funding for this project was provided by SHARCNet, NSERC (R3146-A02), and CIHR (MT 14735, MT 11540, and MGP 49536).