Download
1 / 50
510 likes | 685 Views
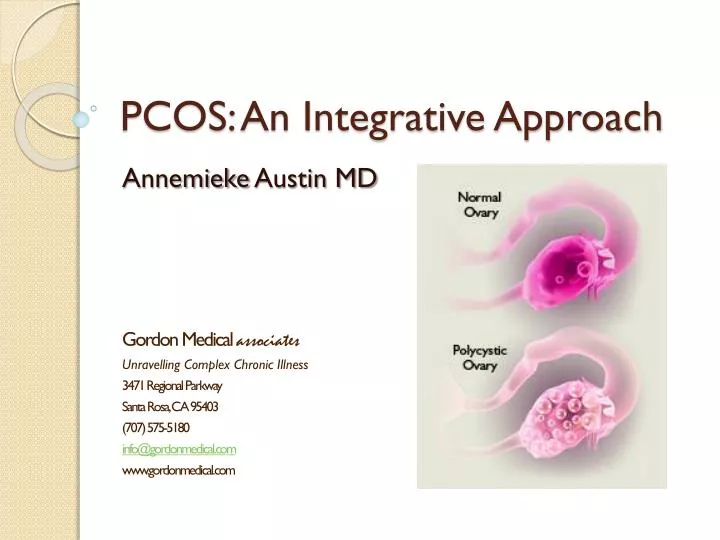
PCOS: An Integrative Approach. Annemieke Austin MD Gordon Medical associates Unravelling Complex Chronic Illness 3471 Regional Parkway Santa Rosa, CA 95403 (707) 575-5180 info@gordonmedical.com www.gordonmedical.com. Martine: a patient example.

E N D
PCOS: An Integrative Approach Annemieke Austin MD Gordon Medical associates Unravelling Complex Chronic Illness 3471 Regional Parkway Santa Rosa, CA 95403 (707) 575-5180 info@gordonmedical.com www.gordonmedical.com
Martine: a patient example • Mid 30’s, trying to get pregnant. Does not want to use fertility treatments because of the risk of having multiple births. • Runs a Marathon every year, trains during the year • 15 lbs overweight around the mid line • Craves sugar, always snacking to prevent herself from getting dizzy • Adult onset acne • Chin hairs – uses electrolysis • Irregular Menstruation
Martine: a patient case • Excess weight around the middle: insulin resistance • Need for constant snacking: unstable blood sugar • Excess Hair: excess testosterone • With lifestyle changes and medication, she was able to have a healthy baby
History • Hipocrates 400 BC described 2 cases of women who developed excess hair growth and whose menses ceased. • Drs Irvin Stein and Michael Leventhal coined the term “polycystic ovary” in 1935 • Dr. Futterweit published the textbook “Polycystic Ovarian Disease” in 1984, considered “the expert”
Epidemiology • 6.5-8% of women overall (Up To Date) • Approximately 6 million women in the United States • 40% have a sister with PCOS, 35% have a mother with PCOS • Very commonly associated or caused by insulin resistance (more on this later)
Symptoms/Clinical Manifestations • Menstrual irregularity 75-80% • Androgen Excess -> 50-90% have increased Testosterone/DHEAS -> hirsutism (excess hair growth), acne, male pattern balding • Infertility due to anovulation • Elevated Insulin Levels (even if not obese) • Increased chance of early pregnancy loss
Symptoms/Clinical Manifestations • Excess weight, sugar craving, inability to lose weight • Abnormal blood lipids (cholesterol) • Apple shaped • Darkening of skin areas around the neck/skin folds • Skin Tags • Gray-white breast discharge • Sleep Apnea • Pelvic Pain associated with cystic rupture • Depression, anxiety, sleep disturbance • Rapid weight change following cessation of BC
Janet’s Story • Health problems started at age 12 • Irregular periods with prolonged bleeding for any years • Depression, uncontrollable hunger, irritability • Weight problems/high cholesterol in her 20’s
Diagnosis of PCOS • Rotterdam Criteria (need 2 out of 3) • 1) Oligo and/or anovulation • 2) Clinical and/or biochemical signs of hyperandrogenism • 3) Polycystic ovaries (on ultrasound) • YOU CAN HAVE REGULAR PERIODS BUT STILL HAVE PCOS
Diagnosis of Insulin Resistance Triglycerides of 150 or greater (100 or less is ideal) Triglyceride/HDL ratio > 3 HDL < 50 Blood Pressure > 130/85 Fasting Glucose of 110 – 125 Fasting insulin > 13 uIU/mL Fasting glucose/insulin ratio < 4/5 Low SHBG: likely due to excess insulin (not accurate if taking birth control)
Pathophysiology/Causes #1: Hyperinsulinemia (Elevated Insulin Levels) • Stimulates androgens (testosterone) production directly in the ovaries • Suppresses SHBG (Sex Hormone Binding Globulin) production in the liver, which increases Free testosterone and estrogen.
Pathophysiology/Causes • In PCOS, the egg follicle does not release the egg into the fallopian tube (no ovulation) • This is likely due to a higher than normal testosterone level. • When eggs are not released they produce “cysts”
Pathophysiology/Causes • Defect in the hypothalamus -> increased LH pulse that stimulates the ovaries to increase secretion of male hormones (LH/FSH ratio increases) • Defect in the ovarian production of testosterone due to abnormal enzyme action • Genetic Causes • Depakote/Valproate medication for epilepsy
Pathophysiology/Causes • PCOS results in progesterone deficiency with excessive estrogen due to lack of ovulation • Estrogen is like the “gas pedal” to the lining of the uterus, making periods heavier -> leads to Dysfunctional Uterine Bleeding • Fat cells also have an enzyme that can increase production of estrogen
Environmental Links/Causes • Bisphenol-A (BPA) has the most research linking it to PCOS and insulin resistance. • BPA has estrogen like effects and can alter other hormones • BPA levels have been found to be higher in women with PCOS, obese or not obese – associated with higher testosterone levels as well • BPA has been found in human tissue, blood, urine, breast milk and fetal blood • It is in plastic food/beverage containers, metal food cans and dental sealants.
Environmental Links/Causes • Phthalates affect menstrual cycles and ovulation. • Phthalates are found in plastics esp in PVC products • Vinyl upholstery, shower curtains, raincoats, children’s toys • DEHP a type of PVC/Phthalate can cause anovulation and disrupts hormones • In men, it has been associated with obesity, insulin resistance
Environmental Links/Causes • Burden of heavy metals has been linked to PCOS • Metals are known to disrupt the menstrual cycle/hormones/fertility • Cadmium, Mercury have been linked with hirsutism, hyperandrogenism, polycystic ovaries. • Arsenic has been linked with insulin resistance and diabetes. • Excess Bromide/Fluoride can be hormonal disrupters.
Metals • Cadmium: found in the soil, water, fertilizer • Mercury: fish, pesticides, wood preservatives, dental fillings, thermometers, fluorescent lights, skin care products, antiseptics, soil, forest fires • Arsenic: chicken, other meats, fish (agricultural fertilizers), Hijiki seaweed, Shellfish, non organic rice, esp rice bran
Risks • Increased risk of endometrial cancer (up to 5 times the risk) -> weight loss and birth control can decrease the risk • Increased risk of cardiovascular disease • Increased risk of diabetes • Increased risk of miscarriage
Testing • Lipid panel Goals: triglycerides <100, HDL > 60, LDL < 100 • Glucose and Insulin tests: Fasting insulin > 13 uIU/mL Fasting glucose/insulin ratio < 4/5 Low SHBG: likely due to excess insulin (not accurate if taking birth control) • Hormones: estrogen/progesterone/testosterone (free & Total), Prolactin, LH, FSH, DHEAS, Androstenedione, Thyroid panel, 17 alpha Hydroxyprogesterone
Testing • If not menstruating: always test thyroid/adrenals (including hyperplasia)/pituitary hormones • Chronic stress/ steroids/extreme exercise/anorexia can also cause problems. • Thyroid disorders, Anemia and low Estrogen can cause hair thinning
Testing/Lab Results • Most women with PCOS have a total testosterone > 60-70 ng/dL • Total Testosterone 70 -150 ng/dL or higher needs further workup • LH/FSH >2 • Prolactin: elevated in 10-20%
Testing for Ovulation • Home kits: tests for LH surge -> ovulation 24 hours later • Basal body temperature: increases by 0.3 to 0.5 F after ovulation -> take at the same time each morning • Progesterone blood level on days 21-23 (most reliable)
Examination • Centrally distributed obesity • Hip/waist ratio of > 0.8 • Look for male pattern hair loss/thinning/texture of the hair • Acne • Abnormal hair growth • Skin changes • Pelvic ultrasound day 4-8 – cysts/uterine lining
Treatment • #1 is diet and exercise • Low glycemic/Low Insulin-emic Diet • High Fiber • Healthy Fats including raw nuts • No fake sugars • No processed foods or flours • Milk has lots of sugar and carbohydrates • Exercise
Conventional Treatment • Metformin: for insulin resistance, regulates menstrual cycle, reduces testosterone levels, weight loss • Before starting metformin for fertility: ultrasound and progesterone treatment (Prometrium 200 mg every night for 7-10 days) • If not ovulating after 2-3 months, will add Clomiphene (together 80% chance of ovulating) • Stop Metformin once you become pregnant • Metformin crosses the placental barrier but studies show no harm
Conventional Treatment: Acne • Mild acne: birth control (suppresses testosterone) • Moderate – severe acne: Spironolactone 50 – 75 mg twice a day -> takes 3-4 months (Take with birth control) • Triple therapy: birth control/spironolactone and metformin • Avoid excess washing and scrubbing • Don’t squeeze pimples • Use non-comedogenic products
Conventional Treatment: Unwanted Hair • Birth control (10% notice improvement) • Spironolactone up to 200 mg per day for at least 6 months • Metformin – maybe but takes 9-12 months for visible improvement • 5 alpha reductase inhibitors (not approved for use in women) Finasteride 2.5-7.5 mg per day -> good for scalp hair loss (Do not get pregnant) • Vaniqa topically
Hair Loss – Male Pattern Baldness • Treat right away – as hair often does not grow back • Spironolactone is most commonly used first line • Can add birth control and finasteride or dutasteride • Rogaine – modestly useful
Treatment - integrative • Again: weight loss, even modest amounts (7-10%) can induce ovulation • Stress management (to decrease cortisol levels) • Diet therapy as discussed previously
Foods that improve insulin • Brassica Family – broccoli, cabbage, brussels sprouts, cauliflower • Green leafy vegetabels • Legumes • Fiber: oat bran, guar gum, psyllium lower post meal insulin • Healthy fats: flaxseed, walnuts, soy, fish, algae
Supplements for Insulin Resistance • Magnesium – check RBC levels Dose: Mag Glycinate or taurate 200-800 mg daily (at night) Chromium has been well studied in diabetes: Chromium picolinate 200-1000 mg daily
Supplements • D-Chiro-Inositol: 1200 mg/day • Increases action of insulin, improved ovulatory function and decreased androgens, blood pressure & triglycerides in women with PCOS • (NEJM 1999:340:1314-1320 Nestler JE) • It is found in buckwheat, not commercially available except for the precursor D-Pinitol by Vital Nutrients • Cheaper alternative: inositol 500 mg twice per day
Other supplements • Vanadium, L- Arginine, Berberine • Berberine has been compared to metformin in studies in diabetes using 500 mg three times a day • “Compared with Metformin, berberine exhibited and identical effect in the regulation of glucose metabolism…. In the regulation of lipid metabolism, berberine is better than Metformin…” • “Efficacy of berberine in patients with type 2 DM” Metabolism, 2008:57 (5): 712-7
And more supplements… • For insulin resistance: • Alpha Lipoic Acid, esp helpful in diabetes with nerve problems: 600-1800 mg/day • Biotin: 2-5 mg • Vitamin C 1000-2000 mg/day (reduces glucose and improves IR) • Omega-3’s – 1-2 tablespoons • Green Tea
Herbs • Panax/American Ginseng before meals 1-3 grams 40 minutes before meals • Bitter Melon 100-200 mg three times/day • Gymnemasylvestre: 400-600 mg/day • Fenugreek: 10-100 gm/day powder away from other meds • Garlic • Saw Palmetto for male pattern balding 450 mg twice per day for 3 months (do not get pregnant)
Maitake Mushroom • Induces ovulation in patients with PCOS • 80 patients: maitake or clomid for 12 weeks to induce ovulation • After 3 cycles, maitake group ovulated 76.9% and the clomid group ovulated 93.5% • Each tab had 18 mg of maitake extract and 250 mg of dried maitake mushroom, 3 tabs three times a day for 3 months • J Altern Complement Med. 2010 Dec; 16(12): 12
Vitamin D and Calcium • Vitmain D deficiency among 13 women with PCOS • Given calcium and vitamin D supplementation (1500mg Ca/day + 50,000 D2/week) • Normalized menstruation and fertility in 9/9 woen with PCOS in 3 months • Thys-Jacobs. Steroids 1999;64(6)
Environmental Cleanup • Eat organic fruits and vegetables (www.ewg.org) • Wild fish, not farmed, and low in mercury • Avoid food stored in plastic • Cans free of BPA: Eden/Vital Choice, some Trader Joes • Organic Meat and Diary to avoid hormones, pesticides and PCB’s • Cook at low temps • Avoid plastic water bottles : avoid numbers: 1,3,6,7. • Do not wrap food in plastic
Water/Air • Water filtration is important to get rid of contaminants like pesticides, herbicides, formaldehyde, detergents, pthalates, PCB’s, Chlorination, lead, copper, PVC • Indoor air: formaldehyde, phthalates from carpet, cleaning products, vinyl flooring, dry cleaning, floor polish, carpet shampoo, air fresheners, mattress, furniture • Consider an air filter
Plants to filter the air • Boston Ferns • Areca palms • Lady palms • Bamboo Palm (solvents) • Rubber plants (formaldehyde) • English Ivy • Dwarf Date Palms • Peace Lillies • Golden Pothos • Dracaena Janet Craig
Beauty and Cosmetic Products • Check the labels • Go to www. organicconsumers.org/bodycare • or skin deep website by the Environmental Working Group: www.cosmeticdatabase.com • www.safecosmetics.org
Detox • Mobilization of pesticides, solvents, fat-loving chemicals: Caloric restriction, Sauna Therapy, Chelation • Sauna is my favorite because it is very effective: up to 10-15 minutes in hot dry sauna at 120-140 degrees followed by 30 second cold shower, repeat 3-4 times as tolerated • Infared may be better tolerated, increase to 30 minutes in the sauna x 2.
Chelation • EDTA/DMPS/DMSA • Selenium, NAC, Alpha Lipoic Acid, Zinc, Modified Citrus Pectin
Liver Detox • Cruciferous vegetables, beets, green tea, pomegranate, flax seed, artichoke, psyllium • Detox supplements: phase 1 and phase 2 liver detox support • Herbs: burdock, dandelion, milk thistle, beet root, artichoke
Estrogen Detox Support • DIM, Calcium – D – Glucarate, NAC, ALA, methylB12, Methyl Folate • DIM is found in cruciferous vegetables • Methylation (B12/folate) • Calcium D Glucarate (cruciferous veggies) allows body to excrete excess estrogen • DIM: metabolite of I3C, improves metabolism of estrogen
Hydrotherapy • Alternating hot and cold shower, 3 minutes hot, 30 seconds cold, repeat 3 times • Epson Salt Bath: 10 minutes follow by 1 minute cold shower • Colon Hydrotherapy
Other Detox support • Castor Oil Packs • High fiber: need regular bowel movements • Probiotics/fermented foods • Coffee enema’s • Drink ½ your body weight in ounces of filtered water each day
Summary • Clean up your diet/air/water • Get rid of chemicals in the home • Sauna • Nutrition most important • A few carefully chosen supplements • Exercise • Stress Reduction • Detox
Contact Dr. Austin Annemieke Austin M.D. Gordon Medicalassociates Unravelling Complex Chronic Illness 3471 Regional Parkway (707) 575 – 5180 info@gordonmedical.com www.gordonmedical.com