Download
1 / 18
210 likes | 1.14k Views
Arterial blood gas interpretation. Larissa Bornikova, MD July, 2006. Objectives. Review the basic pathophysiology of acid-base disturbances. Develop a practical systematic approach to interpretation of acid-base disturbances.

E N D
Arterial blood gas interpretation Larissa Bornikova, MD July, 2006
Objectives • Review the basic pathophysiology of acid-base disturbances. • Develop a practical systematic approach to interpretation of acid-base disturbances. • Understand the clinical application of the A-a gradient in interpreting causes of hypoxemia.
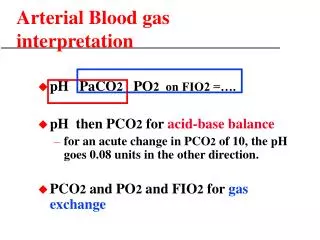
Questions to ask when evaluating ABG’s. • What is acid/base status? • What is the oxygenation status?
Overview Only one equation you must know to understand acid-base problems: HCO3 + H ↔ H2CO3 ↔H20 + CO2 You must understand what effect ventilation has on pH and HCO3 and what effect metabolic disturbances have on ventilation.
Overview (cont’d) The body has three general mechanisms to defend against changes in body fluid pH produced by acid-base disturbances: • Extracellular and intracellular buffering. Instantaneous to minutes. Main physiological buffer systems are CO2/HCO3, phosphate and protein buffer system. • Respiratory defense (adjustments in blood pCO2). Minutes to hours to complete. Chemoreceptors located in the brain and in the periphery (carotid and aortic bodies) sense changes in pCO2 and H+ and alter the ventilatory rate. In metabolic acidosis, pCO2 can be reduced to approximately 10mmHg. In metabolic alkalosis, hypoventilation cannot rise pCO2 above ~ 55 mm Hg (limited by hypoxemia -> stimulator of respiratory drive) * Kussmaul respiration • Renal defense. Takes several days to complete because enzymes need to be synthesized and upregulated. * Acidic urine in contraction metabolic alkalosis
A systematic approach to acid-base • Is the patient acidemic or alkalemic? Action: Determine blood pH (pH <7.38 acidemia; pH >7.42 alkalemia) • Is the primary disturbance metabolic or respiratory? Action: Use CO2 and bicarbonate level to figure out the primary disturbance • If a primary respiratory disturbance is present, is it acute or chronic? Action: Compare measured pH with expected pH • Is compensation appropriate? Action: Compare measured pCO2/bicarb and expected pCO2/bicarb 5. Is there an increased anion gap? Action: Calculate anion gap (AG = Na – (Cl + HCO3)) • Are other metabolic disturbances present in the patient with an anion gap metabolic acidosis? Action: Calculate delta/delta
A systematic approach to acid-base (cont’d) • Is the patient acidemic or alkalemic? Action: Determine blood pH (pH <7.38 acidemia; pH >7.42 alkalemia) • Is the primary disturbance metabolic or respiratory? Action: Use CO2 and bicarbonate level to figure out the primary disturbance • If a primary respiratory disturbance is present, is it acute or chronic? Action: Compare measured pH with expected pH • Is compensation appropriate? Action: Compare measured pCO2/bicarb and expected pCO2/bicarb 5. Is there an increased anion gap? Action: Calculate anion gap (AG = Na – (Cl + HCO3)) • Are other metabolic disturbances present in the patient with an anion gap metabolic acidosis? Action: Calculate delta/delta
A systematic approach to acid-base (cont’d) 3. If a primary respiratory disturbance is present, is it acute or chronic? Action: Compare measured pH with expected pH Acute Resp Acidosis: for every 10 increase pCO2, pH decreases by 0.08 Chronic Resp Acidosis: for every 10 increase pCO2, pH decreases by 0.03 Acute Resp Alkalosis: for every 10 decrease pCO2, pH increases by 0.08 Chronic Resp Alkal: for every 10 decrease pCO2, pH increases by 0.05
A systematic approach to acid-base (cont’d) 4. Is compensation appropriate? Action: Compare measured pCO2/bicarb and expected pCO2/bicarb Metabolic Acidosis Expected pCO2= 1.5[HCO3] + 8 ± 2 Metabolic Alkalosis 10 increase HCO3 : 7 increase pCO2 Resp Acidosis Acute 10 increase pCO2 : 1 increase HCO3 Resp Acidosis Chronic 10 increase pCO2 : 4 increase HCO3 Resp Alkalosis Acute 10 decrease pCO2 : 2 decrease HCO3 Resp Alkalosis Chronic 10 decrease oCO2 : 4 decrease HCO3
A systematic approach to acid-base (cont’d) • Is the patient acidemic or alkalemic? Action: Determine blood pH (pH <7.38 acidemia; pH >7.42 alkalemia) • Is the primary disturbance metabolic or respiratory? Action: Use CO2 and bicarbonate level to figure out the primary disturbance • If a primary respiratory disturbance is present, is it acute or chronic? Action: Compare measured pH with expected pH • Is compensation appropriate? Action: Compare measured pCO2/bicarb and expected pCO2/bicarb 5.Is there an increased anion gap? Action: Calculate anion gap (AG = Na – (Cl + HCO3)) Normal anion gap 12 mEq/L. • Are other metabolic disturbances present in the patient with an anion gap metabolic acidosis? Action: Calculate delta/delta
A systematic approach to acid-base (cont’d) 6. Are other metabolic disturbances present in the patient with an anion gap metabolic acidosis? Action: Calculate delta/delta Delta AG / Delta Bicarb = (12 – AG) / (24 – HCO3) If ratio is ~ 1, pure AG metabolic acidosis If ratio is < 1, suggests concurrent non-AG metabolic acidosis is present If ratio is ≥ 2, suggests that metabolic alkalosis is present
Evaluation of oxygenation. Calculating the alveolar-arterial gradient can help determine whether there is a primary defect in gas exchange or whether hypoxemia is due to extrinsic factors. A-a gradient = PA O2 – Pa O2. A-a gradient = FiO2 (Barometric P – Water P) – (PaCO2)/0.8 – PaO2. A-a gradient = 150 – (PaCO2)/0.8 – PaO2 (under standard conditions) A-a gradient increases with age. Normal ≤ 0.21 x age + 2.5 or age/4 + 2.5 or 0.29 x age
Increased A-a gradient V/Q mismatch (asthma, COPD, alveolar disease, pulmonary vascular disease, PE, pulmonary HTN). R->L shunting (does NOT respond to 100% O2) Decreased diffusion (does NOT respond well to suppl O2) ** Low mixed venous O2 will contribute to hypoxemia in all of the above causes Normal A-a gradient Low inspired FiO2 (high altitude) Hypoventilation. Will always have high PCO2 associated with hypoxemia. There are 5 causes of hypoxemia:
Case I A 38-year-old man with a 2-day history of nausea, vomiting and diarrhea presents to the emergency department because of weakness and dizziness. ABG 7.20/25/ Na = 130 mEq/L; K = 3.2 mEq/L; Cl 80 mEq/L; HCO3 = 10 mEq/L • What acid/base disturbance is present? • What additional laboratory studies you may order for work up of this acid-base disorder? • What conditions may affect the anion gap?
Case II A 22-year-old heroin addict is brought to you comatose. ABG 7.00/80/44 Na = 140; K = 3.2; Cl 80; HCO3 = 20; BUN = 28; Glu = 180 • What acid/base disturbance is present? • What additional laboratory studies you may order for work up of this acid-base disorder? • What is the differential diagnosis for respiratory acidosis in this patient? • What is her A – a gradient?
Case III A 24-year-old man with AIDS presents to the ED with a 5-day history of progressive shortness of breath, cough and fevers. Except for fever, tachycardia and tachypnea his physical exam is normal. CXR is taken. The film is overpenetrated, but appears normal. His oxygen saturation by oximetry is 93% but you ask for an ABG anyway. ABG 7.46/20/60 Na = 129 mEq/L; Cl = 102 mEq/L; HCO3 = 15 mEq/L. • What acid/base disturbance is present? • What is the oxygenation status (A – a gradient)? • What do you suspect is the cause of his symptoms? What additional studies you may consider to order?
Case IV ABG 7.43/46/86 Na = 134 mEq/L; Cl 86 mEq/L; HCO3 = 36 mEq/L. • What is the primary acid-base disturbance? • What is the differential? • What additional tests you may consider ordering to narrow down the potential causes?
References 1. Morganroth, ML. Six steps to acid-base analysis: Clinical applications. The Journal of Crit Ill. 1990; 5; 460 – 469. 2. Up To Date