Download
1 / 98
1.27k likes | 2.66k Views
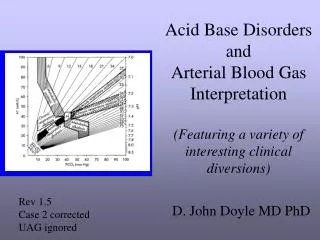
ARTERIAL BLOOD GAS: COLLECTION AND INTERPRETATION. Rey Jaime M. Tan, MD Clinical Associate Professor University of the Philippines College of Medicine. LEARNING OBJECTIVES. Review the ABG collection procedure Recognize the common errors in ABG collection

E N D
ARTERIAL BLOOD GAS: COLLECTION AND INTERPRETATION Rey Jaime M. Tan, MD Clinical Associate Professor University of the Philippines College of Medicine
LEARNING OBJECTIVES • Review the ABG collection procedure • Recognize the common errors in ABG collection • Identify and manage simple and mixed acid-base disturbances • Utilize the serum anion gap in the diagnosis of acid-base disorders
Normal ABG Values ABG INDEX NORMAL VALUE pH 7.35-7.45 paCO235-45 mm Hg paO2 80-100 mm Hg [HCO3] 22 - 26 meq/L SaO2 97-98%
Which of these ABG indices is not directly measured? A. pH B. pCO2 C. pO2 D. HCO3 E. None of the above
Steps in ABG Collection • Prepare the materials needed. • Prepare the syringe with needle. • Select the puncture site. • Perform the modified Allen test. • Collect the sample. • Apply pressure on puncture site. • Prepare the specimen for transport.
Which ABG collection error/s will falsely elevate the pH? A. Failure to cool blood B. Dilution with heparin C. Venous admixture D. Air contamination E. None of the above
Which ABG collection error/s will affect the paO2? A. Failure to cool blood B. Dilution with heparin C. Venous admixture D. Air contamination E. None of the above
Effects of ABG collection errors on pH, paCO2 and paO2 • ABG COLLECTION ERROR pH paCO2paO2 • 1. Dilution with heparin INC DEC NC • 2. Air contamination INC DEC INC • 3. Venous admixture DEC INC DEC • Failure to cool blood DEC INC DEC • Legend: INC=increase, DEC=decrease, NC=no change
Evaluation of Hypoxemia • Room air, patient < 60 y.o. • Mild hypoxemia paO2 < 80 mm Hg • Moderate hypoxemia paO2 < 60 mm Hg • Severe hypoxemia paO2 < 40 mm Hg • For each year > 60 y.o., subtract 1 mm Hg for limits of mild and moderate hypoxemia • At any age, a paO2 < 40 mm Hg indicates severe hypoxemia
Case 1 A 56 year old female vendor developed vomiting and diarrhea 3 days prior to admission. She self medicated with Loperamide, without relief. Her last urine output was 12 hours prior to ER consult. Her BP is 80/60, HR is 110/min. and RR is 28/min. She has poor skin turgor.
Her lab data are as follows: Serum Na = 130 meq/L pH = 7.30 K = 2.5 meq/L pCO2 = 30 mm Hg Cl = 105 meq/L HCO3 = 15 meq/L BUN = 15 mmol/L pO2 = 90 mm Hg Creat = 177 umol/L
What is/are her acid-base disorder/s? • A. simple high AG metabolic acidosis • B. simple NAG metabolic acidosis • mixed metabolic acidosis and respiratory • alkalosis • D. mixed NAG and high AG metabolic acidosis • E. mixed NAG metabolic acidosis and • metabolic alkalosis
STEPWISE APPROACH TO ACID-BASE DISORDERS 1. Obtain diagnostic clues from the clinical setting. 2. Obtain simultaneous ABG and electrolyte profile. 3. Determine the primary disorder. 4. Check the compensatory response. 5. Always calculate the anion gap. 6. Use the delta/deltas when applicable. 7. Look for specific etiologies for the acid-base disorders. 8. Prescribe a treatment regimen.
Vomiting Diarrhea Poor urine output Hypotension Metabolic alkalosis NAG Metabolic acidosis High AG Metabolic acidosis High AG Metabolic acidosis 1. Obtain diagnostic clues from the clinical setting.
Verify ABG using the Henderson equation. • 24 x pCO2 24 x 30 • [H+] = = = 48 • [HCO3-] 15 • Calculate the Na/Cl ratio. • In hydration problems, Na/Cl = 1.4 • In acid-base problems, Na/Cl 1.4 2. Obtain simultaneous ABG and electrolyte profile.
Relationship between arterial pH and [H+] in the physiologic range pH [H+] nanoeq/L 7.80 16 7.70 20 7.60 26 7.50 32 7.40 40 7.30 50 7.20 63 7.10 80 7.00 100
Can venous blood be used to determine acid base disorders? • Venous pH is 0.02 – 0.04 pH units lower than arterial pH • Venous HCO3 is 2 – 3 meq/L higher than arterial HCO3 • Venous pCO2 is 6 – 8 mm Hg higher than arterial pCO2
pH < 7.4 >7.4 acidemia alkalemia HCO3 < 24 pCO2 > 40 HCO3 > 24 pCO2 < 40 metabolic respiratory metabolic respiratory acidosis alkalosis 3. Determine the primary disorder.
URINE Cl- Na+ HCO3- PCT H+ DT normal anion gap Protein- PO4=,SO4= Organic acids NH4+ H2PO4- Regulatory Response to Acidemia
Compensatory Mechanisms • Extracellular buffering primarily by HCO3-(immediate) • Respiratory compensation by an increase in alveolar ventilation (minutes to hours) • Intracellular buffering primarily by proteins and phosphates (2 to 4 hours) • Renal compensation by an ↑ in H+ excretion and ↑HCO3- reabsorption (hours to days)
Henderson-Hasselbalch equation: HCO3 pH = 6.1 + log 0.03 x pCO2 HCO3 pH = 6.1 + log 0.03 x pCO2 HCO3 pH = 6.1 + log 0.03 x pCO2
Henderson Equation 24 x pCO2 [H+] = [HCO3-] 24 x pCO2 [H+] = [HCO3-] 24 x pCO2 [H+] = [HCO3-]
4. Compute for the compensatory response. • HCO3 = 24 – 15 = 9 pCO2 = 9 x 1.2 = 10.8 Exp. pCO2 = 40 – 10.8 = 29.2 ± 2 Actual pCO2 of 30 is within the exp. pCO2 This is a simple metabolic acidosis
SERUM ANION GAP Na - [Cl + HCO3] = 12 ± 4 TC = TA MC + UC = MA + UA MC - MA = UA - UC = anion gap Na - [Cl + HCO3] = UA - UC = anion gap UA: Lactate, Ketones, Uremic anions, Toxic anions, Albumin UC: Potassium, Calcium, Magnesium, Globulin, Lithium
5. Calculate the anion gap. AG = Na – [Cl + HCO3] = 130 – [105 + 15] = 10 This is a simple normal anion gap metabolic acidosis. Note: A high AG ALWAYS indicates the presence of a high AG metabolic acidosis.
Na 136 Cl 100 Na 136 Cl 100 Na 136 Cl 106 Na 136 Cl 94 HCO3 20 HCO3 14 HCO3 24 HCO3 8 AG 12 AG 22 AG 22 AG 22 NORMAL SIMPLE AG METABOLIC ACIDOSIS AG HCO3 COMBINED AG & NAG MET. ACIDOSIS AG HCO3 COMBINED AG MET. ACIDOSIS & MET. ALKALOSIS AG HCO3 10 10 10 16 10 4 = = = DELTA AnionGap/DELTA HCO3
Na 136 Cl 100 Na 134 Cl 110 Na 128 Cl 110 Na 140 Cl 110 HCO3 24 HCO3 20 HCO3 14 HCO3 8 AG 12 AG 10 AG 10 AG 10 NORMAL SIMPLE NAG METABOLIC ACIDOSIS Cl HCO3 COMBINED NAG & AG MET. ACIDOSIS Cl HCO3 COMBINED NAG MET. ACIDOSIS & MET. ALKALOSIS Cl HCO3 10 10 10 16 10 4 = = = DELTA Chloride/DELTA HCO3
Cl 105 –100 5 HCO3 24 – 15 9 = = 6. Use the delta-deltas to detect coexisting metabolic disorders. This is a combined normal anion gap and high anion gap metabolic acidosis.
CAUSES OF METABOLIC ACIDOSIS • INCREASED ANION GAP • Ketoacidosis • Diabetic • Alcoholism • Starvation • Lactic Acidosis • Uremia • Toxins • NORMAL ANION GAP • Associated w/ K loss • Diarrhea • RTA • Interstitial nephritis • Early renal failure • Urinary tract obstrxn • Drug-induced
Cl- M- methanol U- uremia D- DKA P- paraldehyde I- iron, INH L- lactic acidosis E- ethylene glycol S- salicylates Na+ HCO3- H+ High anion gap Protein- PO4=,SO4= Organic acids States of Systemic Acidosis
How would you correct her acid-base disorder? A. KCl infusion B. Intravenous NaHCO3 drip C. Oral NaHCO3 D. Hydration alone
Na content Na meq/mL mosm/L 0.9% saline 0.15 308 7.5% NaHCO3 0.89 1784 8.4% NaHCO3 1.00 2000 COMPLICATIONS OF HCO3 THERAPY • Causes volume overload/hypernatremia/ hyperosmolality
COMPLICATIONS OF HCO3 THERAPY • Worsens hypokalemia and hypocalcemia • Induces intracellular acidosis • Causes overshoot alkalosis • Stimulates organic acid production • Decreases tissue oxygen delivery
BENEFITS OF HCO3 THERAPY • minimizes depletion of buffer stores by ongoing metabolic acidosis • reverses the harmful cardiovascular effects of systemic acidosis (decreased cardiac output, decreased arteriolar resistance, increased venoconstriction)
Pure LA LA + mild worse LA HCO3 Tx CO2 retention for pure LA pH 7.15 7.06 6.70 7.35 pCO2 15 18 15 15 HCO3 5 5 2 8 BENEFITS OF HCO3 THERAPY • in severe acidemia, systemic pH is sensitive to small absolute changes in pCO2 and HCO3
GENERAL INDICATIONS FOR HCO3 THERAPY • pH < 7.20 and HCO3 < 5 - 10 mm Hg • Used when inadequate ventilatory compensation is present • Elderly on beta blockers in severe acidosis with compromised cardiac function • Concurrent severe AG and NAG metabolic acidosis • Severe acidemia with renal failure or intoxications
Case 2 A 30 year old male with a history of epilepsy has a grand mal seizure. Laboratory tests taken immediately after the seizure has stopped reveal: Arterial pH = 7.14 pCO2 = 45 mm Hg Plasma [Na+] = 140 meq/L [K+] = 4.0 meq/L [Cl-] = 98 meq/L [HCO3-] = 17 meq/L AG = 25
What is/are his acid-base disorder/s? • A. simple high AG metabolic acidosis • B. simple NAG metabolic acidosis • mixed metabolic acidosis and • respiratory alkalosis • mixed metabolic acidosis and • respiratory acidosis
STEPWISE APPROACH TO ACID-BASE DISORDERS 1. Obtain diagnostic clues from the clinical setting. 2. Obtain simultaneous ABG and electrolyte profile. 3. Determine the primary disorder. 4. Check the compensatory response. 5. Always calculate the anion gap. 6. Use the delta/deltas when applicable. 7. Look for specific etiologies for the acid-base disorders. 8. Prescribe a treatment regimen.
Seizure Depressed sensorium Lactic acidosis HAG metabolic acidosis Respiratory acidosis 1. Obtain diagnostic clues from the clinical setting.
Case 2 A 30 year old male with a history of epilepsy has a grand mal seizure. Laboratory tests taken immediately after the seizure has stopped reveal: Arterial pH = 7.14 pCO2 = 45 mm Hg Plasma [Na+] = 140 meq/L [K+] = 4.0 meq/L [Cl-] = 98 meq/L [HCO3-] = 17 meq/L AG = 25
3. Determine the primary disorder. pH < 7.4 >7.4 acidemia alkalemia HCO3 < 24 pCO2 > 40 HCO3 > 24 pCO2 < 40 metabolic respiratory metabolic respiratory acidosis alkalosis
pCO2 40 HCO3 24 vs. 45 - 40 40 24 - 17 24 vs. 5 40 7 24 > The primary disorder is a metabolic acidosis.
4. Compute for the compensatory response. • HCO3 = 24 – 17 = 7 pCO2 = 7 x 1.2 = 8.4 Exp. pCO2 = 40 – 8.4 = 31.6 ± 2 Actual pCO2 of 45 is higher than exp. pCO2 This is a mixed metabolic acidosis and respiratory acidosis.
AG 25 – 12 13 HCO3 24 – 17 7 = = 6. Use the delta-deltas to detect coexisting metabolic disorders. This is a combined high anion gap metabolic acidosis and metabolic alkalosis.
How would you correct his acid-base disorder? A. administer IV NaHCO3 using HCO3 deficit B. administer oral NaHCO3 at 1 meq/kg/day C. Intubate D. no treatment
Compute HCO3 deficit. HCO3 deficit = [Desired HCO3 – Actual HCO3] x 0.5* x kg BW * As the serum HCO3 decreases below 5-10, the volume of distribution increases and total HCO3 requirement will also increase use 0.7 – 1.0 Maintenance HCO3 = 1 meq/kg/day
Principles of HCO3 therapy in lactic acidosis • Primary effort should be directed at improving the delivery of oxygen • Use NaHCO3 only when HCO3 < 5 mmol/L • In states of low cardiac output, raising the cardiac output will have a larger impact on the pH of the ICF than will HCO3 therapy • In cases with low alveolar ventilation, increase ventilation to lower the tissue pCO2
Principles of HCO3 therapy in ketoacidosis • In ketoacidosis, the rate of H+ production is slow and NaHCO3 therapy may carry the risk of provoking severe hypokalemia, NaHCO3 should be avoided in most cases • Consider HCO3 therapy: • Severe hyperkalemia despite insulin • When HCO3 < 5 mmol/L • Worsening acidemia inspite of insulin