Download
1 / 20
220 likes | 287 Views
Teaching Clinical Pathology of Disorders of RBC covered using a clinical case of Anemia. Pathology lecture and tutorials are delivered through short video clips covering parts of topic. this is the first part with overview of whole topic and clinical case. Each powerpoint is screen recorded using camtasia studio and saved as MP4 video.

E N D
Any fool can know. The point is to understand ! -- Albert Einstein Know Pathology – you know medicine. Without Pathology, Medicine is quackery…!
CLINICAL PATHOLOGY The foundation of Clinical Medicine. Shashidhar Venkatesh Murthy A/Prof & Head of Pathology College of Medicine & Dentistry RBC Disorders: Introduction
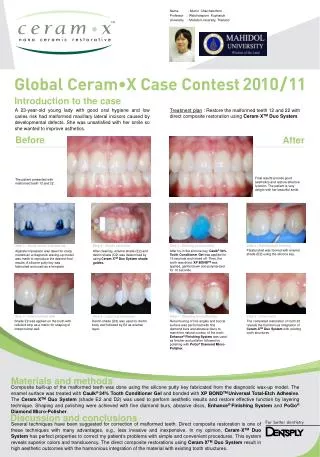
CPC 2.1: Tired woman... 63y Ayr – Increasing lethargy, dyspnea, edema - 1year Difficulty walking – weakness & unsteadiness. - 2week Initially treated with iron tablets. Increasing lethargy, SOB, dyspnea, ankle swelling… Palpitations, chest pain on exertion, relieved on rest. Fever some times. Loss of appetite, some loss of weight Hypothyroidism- thyroxine, NSAID for osteoarthritis. Bruises easily, Pale, mild jaundice. Stomatitis, glossitis, PNS: 4/5 lower limb, Romberg +ve, Reflexes , Babinski +ve, sensation Differntial Diagnosis: Megaloblastic anemia Pernicious anemia Hypothy. – macro. An. Malignancy, Aplastic, Refractory anemia. GI bleeds,
CPC scenarios: 2014: I.H. 16 year old girl from Bamaga; attending boarding school in Charters Towers Presents to GP: “I’m feeling very short of breath when I play netball”. Accompanied by boarding house teacher (female) 2012: Mrs. IS, 68y old pensioner, rural near Ingham. Husband, a butcher. She is on warfarin for 10y, for atrial fibrillation. HPTN on Aldomet. She feels tired and is pale yellow and gets angina while going for a regular evening walk. What if “The patient” is a …? • 64y woman (occult GI loss, hypothyroidism, chronic disease) • 40y woman (mennorhagia) • 40y man (occult malignancy, haematological malignancy) • 65y man with Stage 4 renal failure (discuss renal anaemia) • 74y man with no PMH of note (B12 def., occult GI malignancy)
CPC2.1: Tired woman: Lab results: 1. Where is the primary pathology (diagnosis?) 2. What psychiatric symptoms in Vit B12 deficiency? 3. FBC in AHA, MBA, IDA, ACD, Acute / Chronic blood loss?
“Success is going from failure to failure without loss of enthusiasm” ! – Winston Churchill
CPC 2.1: RBC disorders 2014 Term 2 CPC 1 System: Aim: Title: Haematopoetic 1/2 Anaemia Haematopoietic system To educate students in: Clinical, pathological & population studies of patients with anaemia (RBC disorders) Objectives: 1. Demonstrate competency in history taking & clinical examination of patients with anaemia and related illnesses. 2. Describe the pathophysiology of the acute anaemic process and the common causes and important other rare causes of anaemia, particularly in the tropics and Indigenous populations. 3. Outline the basic sciences relating to bone marrow, red blood cell production and turnover of iron, routine blood test parameters, measurement of iron stores, and precursors important for red cell production. 4. Demonstrate an understanding of the complications of anaemia and anaemia as a presentation for other pathologies and as an illness in itself. MB2:HRM: Week 2&3 RBC
Learning Objectives: Diseases of RBC Anaemia: Overview, Classification, pathogenesis, diagnosis, clinical features & complications. Study TOP 10 ANEMIA Major (detailed) Iron Deficiency anemia. Megaloblastic anemia. Imm. Hemolytic (Warm/Cold) Anemia of Chronic Disease. Aplastic Anemia Minor (brief note) Myelodysplastic/Refractory An Sickle Cell Anemia Thalassemia syndromes. G6PD deficiency anemia. Hereditary Spherocytosis. 1. 2. 3. 4. 5. 1. 2. 3. 4. 5.
Whatever you think, that you will be. If you think yourselves weak, weak you will be. If you think yourselves strong, strong you will be! -- Swami Vivekananda
CLINICAL PATHOLOGY The foundation of Clinical Medicine. Shashidhar Venkatesh Murthy A/Prof & Head of Pathology College of Medicine & Dentistry RBC & Anemia: Pathophysiology
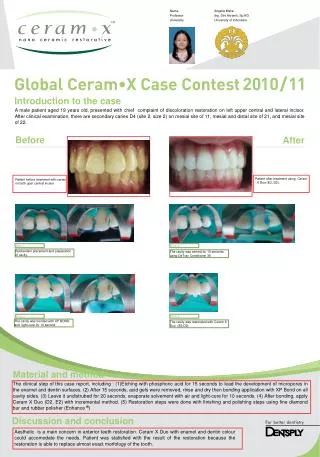
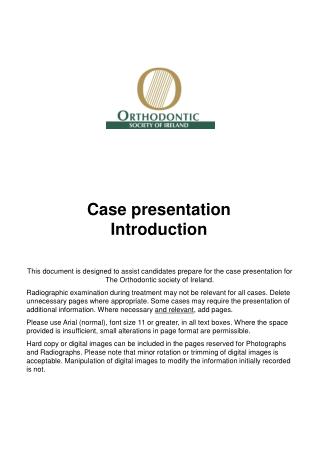
Reticulocyte (immature) MCV >100 Normal RBC 8 μ 8 μ Persisting RNA Retic. Band 8 μ L 12-14μ N Capillary 5-10 μ Only healthy elastic RBC can squeeze through capillary. RBC Histogram
Definition of Anemia: “Anemia is decreased red cell mass affecting tissue oxygenation” Diagnosed using Hematocrit or Hb. levels (Low Hb* or Low HCT) Types: Decreased production – Deficiency anemia. Increased loss/destruction – Hemolytic anemia. 12
Pathogenetic Classification of Anemia: Top 6 Anemias: 1. Iron Def. A 2. Megaloblastic 3. Anem. Of Chronic Dis. 4. Aplastic An. 5. Immune Hemolytic – Warm 6. Immune Hemolytic - Cold Decreased Production: Nutrient Deficiency. Iron def (IDA) / Megaloblastic (MBA) Hemopoietic cell defect: Anemia of chronic disorders (ACD) Aplastic anemia (AA). Dysplastic anemia. Myelodysplastic Syndromes Increased loss / destruction: Blood loss anemia – Acute / Chronic - bleeding. Hemolytic anemia – Congenital / Acquired. Acquired / External injury. Immune AIHA (Warm/Cold) Mechanical, Drugs & Parasites Congenital / Internal RBC defect Defective Membrane (Spherocytic an) Defective Hemoglobin (Sickle cell an.) Deficient Enzyme (G6PD) 2 2 2 •Cell Mem •Hb. •Enzymes
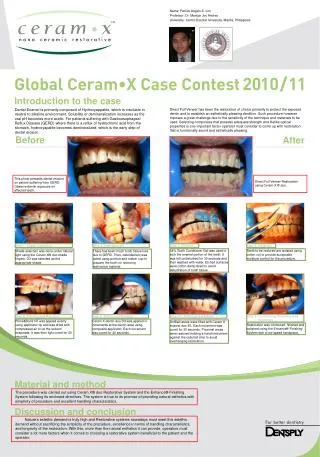
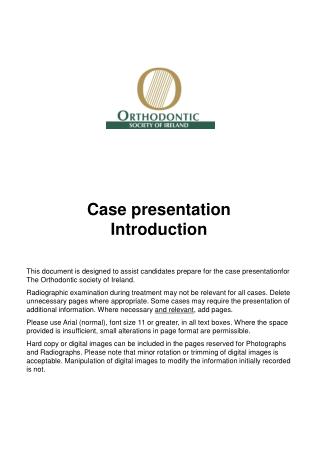
RBC development: MCV 110 MCV 90 Bone Marrow 14
Anemia Pathogenesis: Megaloblastic anemia DNA: B12, Folate BLAST Early Intermediate Retic. RBC Late Aplastic anemia Dysplastic anemia Hemolytic anemia Immune Mechanica l Infection Drugs Defective* Proerythroblast (Pronormoblast) Polychromatophilic Normoblast Reticulocyte Basophilic Normoblast Orthochromatophilic Normoblast Erythrocyte Iron Deficiency anemia Hb: Iron Iron Metabolism: “limited”,10%, Recycle, Ferritin, Transferrin, Hepcidin, forms Hb in cytoplasm.
We are here for you…. venkatesh.shashidhar@jcu.edu.au (Shashi) Daisy.mehra@jcu.edu.au (Daisy) Need personal help? Email us for an appointment or call, Office Tel: 4781 4566 (Shashi) Office Tel: 4781 5626 (Daisy)
When your thinking is brilliant, you will be brilliant, but if your thinking is not brilliant you will not be brilliant, no matter how brilliant you may think you are….! -- Christian D. Larson Fake it until you make it…! -- Mohd. Ali. Boxer.