Download
1 / 39
420 likes | 566 Views
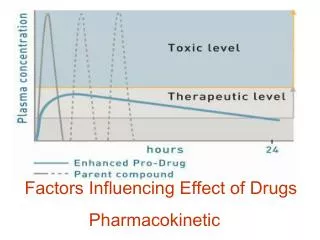
Drug Dosage Forms . Factors Influencing Effects of Drugs. Original vs . Generic drug.

E N D
Originalvs. Genericdrug Originaldrug (Brand namedrug)– a drug on the market thatcontainsmedication not knownbefore. Itisprotectedseveralyears by patent, since a companyspentmoney on research, marketing and promotion. Genericdrug –is a drugwithout patent protection. Contains the same effective substances, but may contain different additive substances. Needs to bebioequivalent to thebrandnamedrugwithrespect to pharmacokinetic and pharmacodynamicproperties. Theadvantageisespeciallytheprice.
Originalvs. Genericdrug– bioequivalence • There is a common misperception that generic drug concentrations can be 80% to 125% of the brand name formulation; in other words, that the variance may be up to 45%.Nottrue. • One of the key parameters for bioequivalence is the area under the curve (AUC). The AUC is a mathematical calculation based on a graph of blood concentration versus time. • The AUC of a generic formulation must be no less than 80% or no more than 125% of the brand name formulation. There is international consensus that differences within this range are not clinically significant. • More importantly, the 90% confidence interval of the AUC must also fall within 80% to 125%. Recall that the confidence interval is a range of measurements within which we can be confident that the true result lies. So, for the entire confidence interval to fall within the 80% to 125% range, the variance is generally less than 5%. • According to: Canadian Agency for Drugs and Technologies in Health
Differencebetweensmallmolecule/genericdrugsvs. biologicdrugs/biosimilars? Smallmolecule/ generic drugs Biologicdrugs/ biosimilars • Highermolecular weight • Usually less stable at room temperature • Usually administered parenterally • Made out of cells or organisms through biotechnology • A heterogeneous product, which is difficult to standardize • Often at higher risk of immunogenicity • Low molecular weight • Stable at room temperature • Usually administered p.o. • Organical / chemical synthesis • A homogeneous product of high purity with the established standards • Known structure • Rare immunogenicity
Biologicdrugs/biosimilars • Devidedinto: • Proteinsalmostidenticalwithproteinssynthetised in our body. Used as substitutiontherapy or to increaseproductionotthesesubstances by organismitself (insulin, growthhormone or erythropoetin). • Monoclonalantibodies, that bind to soluble or surface proteins of the cells to block specific metabolic pathways of cells. • Artificiallycreatedproteinsthatmimicreceptors (soluble receptors and receptor antagonists), but they are soluble and designed to be stable in the human body. • Living microrganisms or like particles(viruses and bacterias), virulence of which is controlled (vaccines).
Drug - composition • activecomponents (responsiblefortheeffect) • inactivecomponents (excipients) – e.g. tablets: • diluent (providing extra volume for the tablet) • binder(substance that holds the tablet together) • disintegrant(helps the tablet break apart and dissolve in the GI tract) • lubricant(substance thatprevents wear and tear on the tablet making equipmentand makesit easier to remove the tablet from a mold) • may also contain additional ingredients such as sweeteners and/or coloring agents
Ways of administration Wayofadministrationisthewaythroughwhichdrugreachesorganism. Wayofadinistrationdepends on drugform, physical and chemicalpropertiesofthedrugandpsysicalandmental state ofthepatient. Ways of administration are divided to local (topic) and systemic. local Administration systemic enteral Administration parenteral
Drug dosage forms can be divided according to consistency to liquid, solid, semisolid and aerosols. Drug dosage forms can also be set for internal or external use.
Soliddosageforms • tablets (bucal, sublingual, chewable, effervescent, film-coated, controlled-release = prolonged-release (PR) or sustained-release (SR)) • capsules (hard gelatin = dry-filled, soft elastic = the contents may be liquid, paste,or powder, enteric-coated) • pills (small round dosage forms prepared by pharmacist, now rarely used) • troches (lozenges or pastilles; they are placed in the mouth where they slowly dissolve) • powders • granules(particularly suitable for the preparation of solutions or mixtures of drugs, that are unstable in the presence of water)
Tablets • tablets are supplied in many shapes, sizes, and colors • the most common type of tablet is made by compression or molding and is intended to be swallowed whole • chewable tablet meant to be chewed before swallowing (e.g. children) • enteric coated tablet allows a tablet to pass through the stomach to be broken down and absorbed in the intestine • effervescent tablets are designed to be dissolved in water • buccal tablets are designed to be dissolved in the mouth between the ch • sublingual tablet is dissolved under the tongue.eek and gum (e.g. nitroglycerin) • lozenge (troches/pastilles)is a tablet designed to be slowly dissolved in the mouth or upper throat (e.g. many OTC "sore throat" medications) • orally disintegrating tablets & films
Capsules • a gelatin or methylcellulose shell • 2 types: the hard capsule intended to contain solids, and the elastic or soft capsule designed to hold liquids • advantages: uniform and clean, effectively mask the odor and taste of drugs, provide an accurate dosage, rapid release of medication in the stomach • capsules should be dispensed in glass or plastic containers that protect them from moisture and dust
Other solid dosage forms • Pillwas originally defined as a small, round, solid pharmaceutical oral dosage form of medication that was in use before the advent of tablets and capsules. • Powder is a dry, bulk solid composed of a large number of very fine particles. • Granules - granulation process transforms fine powders into free-flowing, dust-free granules that are easy to compress.
Tablets and Capsules - Time Release or Extended Release Technologies – „retard“ tbl. • to allow a drug to dissolve over time in order to provide a steady release into the bloodstream, and reduce the need for frequent dosing: • SR - sustained release • SA - sustained action • ER, XR, XL - extended release • TR - timed release • CR - controlled release • MR - modified release e.g. of an extended release system: tablet that employs osmotic pressure to deliver drug at a zero order rateindependentlyof pH or intestinal motility;incorporation of the drug into a waxy matrix or within a polymer that slowly dissolves and releases the drug for subsequent absorption
Semisolid dosage forms • Cream (emulsion bases, contain a water phase) • Gels (high degree of clarity, ease of application and ease of removal and use; active ingredients are incorporated into water-soluble bases) • Ointment (oleaginous bases, most often contain vaselinum or parrafinum liquidum) • Paste (forms containing large amounts of solids) • Suppositories (rectal, vaginal) • Transdermal patch (antianginal, analgesic, steroidal drugs)
Semisolid dosage forms – made more simple • CREAM (oil in water emulsion) • OINTMENT (water in oil emulsion) • LOTION (oil in water emulsion that is thinner than cream) • GEL (contains solid medication particles, like suspension, in a thick liquid) • PASTE (contains more solid material)
Suppositories • intended for insertion into a body cavity or orifice other than the mouth (e.g. rectal or vaginal) • the vehicle either melts or dissolves following insertion. • they are used for local effect (e.g. as a laxative, or treatment for colitis) or for systemic absorption when the individual cannot easily take medication orally (e.g., vomiting or unconscious).
Transdermal Patch • rapidly developing dosage formulation for topical application of medication for systemic absorption • they look very much like a band-aid • estrogenplus progestincontraceptive • fentanylpatchforpain management • nicotinepatchfor smoking cessation • nitroglycerinpatchforanginapectoris
Liquiddosageforms • Prepared by dissolving the active ingredients in an aqueous or nonaqueous solvent: • Solutions(homogeneous mixtures that are prepared by dissolving a solid, liquid, or gas in another liquid) • Emulsions(two-phase systems in which one liquid is dispersed throughout another liquid in the form of small droplets) • Suspensions(two-phase systems consisting of finely divided solids dispersed in liquids) • Ways of application: • Syrups • Drops (eyedropscan´tbeopened more thanonemonth) • Enema • Injections (i.v., i.m., s.c.) • Infusions
Advantages of liquid dosage forms • Pediatric patients • Geriatric patients • Patients with feeding tube • Onset of action faster than with solid drug forms
Disadvantages of liquid dosage forms • Loss of effect sooner than with solid drug forms • Difficult to mask taste or odor • Potential for dosing innacuracy • Incovenient
Liquid dosage forms - aqueous • these dosage forms are less stable and have a shorter shelf life than other dosage forms • children under the age of 10 years old commonly cannot swallow tablets, and dislike injections • Solutions- the most accurate way to give a variable dosage. Color and flavor can be used to enhance acceptance. • Suspensions- consists of a dispersion of tiny undissolved drug particles suspended in the solution. Needs to be shaken. • Syrup -containing a high concentration of a sugar (or sugar substitute), a flavoring agent, and active drug ingredients. Often use cherry or chocolate taste.
Liquid dosage forms – with alcohol • Fluid extract - in which 1 ml represents the extractable ingredients for 1 g of a plant-derived drug • Tincture - in which 10 ml represents the extractable ingredients from 1 g of crude drug • Elixir - also sweetened solutions, but a bit less sweet and viscous than syrups. They also contain alcohol.
Injections • are among the most common health care procedures • intradermal, subcutaneous, intramuscular, intravenous, intraosseous, intraperitoneal, intrathecal, epidural, intracardiac, intraarticular, intracavernous, and intravitreal • long-acting forms of subcutaneous/intramuscular injections (depot injections)
Injections - i.v. injections or infusions • all drugs administerd i.m., i.v., s.c. must be sterile • used to deliver antibiotics, analgesics, i.v. fluids, nutritional supplements • usually administered into the vein of the arm • most parenteral preparations are prepared in a sterile-water, normal saline or other solutions
Injections - i.m. injections • Can be used to deliver small volume of medication • Antibiotics, analgesics, vitamins, some vaccines • Usually administered into upper outer portion of the buttock • In children can be also given in the deltoid muscle of the shoulder • Administered at 90 degree angle
Injections – s.c. injections • Can be used to deliver small volume of medication • Usually administered at lower part of abdomen, top of the thigh, outside of the upper arm • Administered at 45 degree angle, in lean or obese closer to 90 degree angle
Aerosols = Gaseousdosageforms • These drugs are designed to carry the drug into the respiratory tract, on the skin and mucous membrane • Inhaler (asthma, otherrespiratorydiseases; everyday use) • Nebulizer (device to administermedication in formof a liquidmist to airways; used more in hospital)
Aerosols = Gaseousdosageforms The most common medical indications: asthma or chronic obstructive pulmonary disease (COPD) The most common drugs: β-2 bronchodilators, anticholinergics or corticosteroids Also inhalational anesthetics
Orphan drug • are intended to treat diseases so rare that sponsors are reluctant to develop them under usual marketing conditions • thesediseases affect only a small proportion of the population (less than one person per 2,000 in Europe), most often at birth or in infancy. According to: Orphanet (theportalforrarediseases and orphandrugs)
Orphan drug • InEuropeanunionweresince2010 registered59 orphandrugsfromwhich: • 45,8 % orphandrugsforrareoncologicdiseases • 20,3 % forrarediseases of GIT and metabolism • 11,8 % forrareneurologicdiseases • 8,5 % forrarecardiovascular and otherdiseases
FactorsInfluencingEffectsofDrugs • external • characteristic of the drug, way of application, doses and their intervals... • they can be easily changed • internal • patient´s characteristic (age, gender,...) • change is impossible or very problematic
ExternalFactors – RoutesofAdministration Medicationscanbeadministered by differentroutes Theselectionisofteninfluenced by age and condition The oral routeisthe most commonroute PERORAL ADMINISTRATION Peroral/oral route Safe, easy, medications are usuallylessexpensive Canbeinfluenced by presenceofothersubstances: drugs (antacids, prokinetics, contentofions – possiblechelation), food (possiblechangeofabsorption) Sublingual/buccal PARENTERAL ADMINISTRATION I.v. route Bolusdose or constantinfusion I.m. route Ifneededfasteffect, ifthedrugdissolves in GIT (penicilin G), ifhigh „firstpasseffect“ (lidocain), ifbadcompliance Influenced by liposolubility, pH ofsolution, muscleperfusion S.c. and i.d. route
ExternalFactors – RoutesofAdministration TOPICAL APPLICATION = to thesurfaceofthe skin or mucousmembranes Theeffectcanbesystemic or local LessADRs, rapidaction Maycause skin irritation Transdermal: plasters, gels (nitroglycerin, fentanyl,...) Ophtalmic, Otic, Nasal (alsopeptides – vasopressin, calcitonin) Rectal Fasteffect, low „firstpass“ No irritationofstomachmucousmembrane Ifpatientcan´ttakedrugs per os Vaginal, urethral Inhalation Inhalationofgas, aerosol, particles Quickeffect
External Factors – Dosing Time of Application Chronopharmacology • glucocortikoids, digoxin, ciklosporin, antihypertensives, insulins In case of all drugs, the best is if they are taken around the same time intervals (especially important with antibiotics) Xenobiotics, drugs a chemical compound (such as a drug, pesticide, or carcinogen) that is foreign to a living organism
Internal Factors - Age CHILDREN • To determine the dose can be used: body-surface area (the best way to calculate dose), age, body weight (the most often used since it is easy to obtain) • Always check the calculations of dosages! • Differences in pharmacokinetics compared to adults: • Absorption (↓ volume of gastric and duodenal liquid, ↓ acidity, ↓ absorption surface) • Biotransformation (immaturity of enzyme systems) • Bigger extracelular space • Incorporation of drug to growing tissues (tetracyclines) • ↓ glomerular filtration
Internal Factors - Age GERIATRIC PATIENTS • Differences in pharmacokinetics compared to adults: • ↓ acidity, slower motility, longer time to evacuate stomach, venostasis in the splanchnic region • ↓ activity of biotransformating enzymes, ↓ perfusion of liver • ↓ concentration of binding proteins • ↓ weight of the body, slower circulation • ↓ of kidney function Polypharmacy = concurrent use of multiple medications Noncompliance = failure to adhere to the prescribed drug regimen (common in elderly and children, patient can get written information and dosing aids – e.g. pillbox)
Internal Factors - Gender WOMEN • ↓ absorption surface • Competition of estrogens and progesteron with metabolism • ↓ glomerular filtration, ↓ weight, ↑ ratio of body lipids • Choice of drugs with respect to gravidity and lactation
Internal Factors – Patologic State absorption • GIT diseases (quicker or slower pasage, surgery, inflammation in the area of application) distribution • states connected with hypoalbuminemia (nephrotic syndrome, deffect of proteosynthesis in liver) biotransformation • diseases of liver parenchyma (changes of metabolisation, presystemic elimination) excretion - kidney deffects, changes of inner space
Internal Factors – Genetic Factors genetically dependent changes: • pharmacodynamics - resistance to cumarines, decreased effect of β-blockers among afro-americans • pharmacokinetics - biotransformational polymorfism (slow, fast acetylators, hydroxylators)