Download
1 / 89

E N D
Cardiac Physiology Heather Hale SPEP 2009
“…it is nearly impossible to contemplate the pumping action of the heart without being struck by its simplicity of design, its wide range of activity and functional capacity, and the staggering amount of work it performs relentlessly over the lifetime of an individual…” Berne and Levy, Principles of Physiology 4th ed., Elsevier
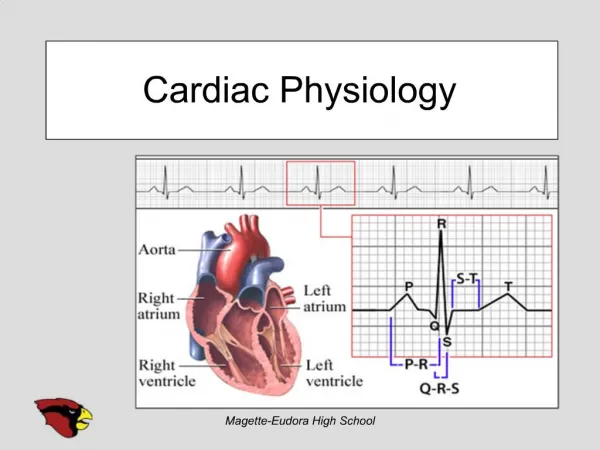
Overview • The heart as a pump: • Functional anatomy • Nervous system influence • Effective cardiac pumping • Action potential propagation in the heart • Pressure-volume relationships • Electrocardiogram readings
What does the heart really do? • A lot!!! • Main function: serve as a reciprocating pump that develops the necessary pressure gradients to circulate blood throughout the vasculature
Cardiac Physiology Cardiac pump cycle
The heart is composed of two pumps in series “Right heart” - Pumps blood through pulmonary circuit “Left heart” - Propels blood through the peripheral (systemic) circulation Both sides are composed of two chambers Atrium - smaller chamber Ventricle - large chamber The right and left sides are not directly connected to each other, but the chambers within each side are connected How does it work?
Blood flow through the heart • Systemic blood (tissues/ muscles/organs) uses O2 • De-oxygenated blood returns to right heart • Blood is pumped from right heart to lungs • Gas exchange occurs • Re-oxygenated blood returns to left heart • Blood is pumped from left heart back to body Video: Blood flow through the heart http://www.sumanasinc.com/webcontent/animations/content/human_heart.html
Functional anatomy: right heart • Receives systemic (deoxygenated) blood through vena cava • Blood flow: Right atrium (tricuspid valve) Right ventricle (pulmonary valve) Pulmonary artery Lungs
Functional anatomy: left heart • Receives (oxygenated) blood from lungs through pulmonary vein • Blood flow: Left atrium (mitral valve) Left ventricle (aortic valve) Aorta Body
Valves are critical to maintain unidirectional blood flow Functional anatomy: valves • Atrioventricular valves (AV valves) • Present between each atrium and ventricle • Tricuspid + mitral valves • Semilunar valves (SL valves; “outlet” valves) • Present between ventricle and outlet • Pulmonary + aortic • Open/close passively in response to pressure
Functional anatomy: valve defects • Detected as heart murmurs • Abnormal heart sounds (auscultations) • Created by abnormal blood flow patterns • Types of valve defects • Stenotic = failure to open fully (narrowing) • Regurgitant = failure to seal upon closure • These can happen at the same time!
Neural influences on heart • Some intrinsic rhythmicity exists, but the heart is also influenced by the autonomic nervous system • Sympathetic influences: • Adrenergic receptors (respond to norepinephrine) • Increases heart rate and pumping • Parasympathetic influences: • Cholinergic receptors (respond to aceylcholine) • Decreases heart rate and pumping
Cardiac pump cycle • Pumping is necessary to cyclically change blood in each chamber • Cycle is rhythmic and synchronized • Two major phases: • Diastole • Systole • Both are defined by action of the ventricle!
Filling stage Ventricular relaxation Blood flows down pressure gradient from atria to ventricle AV valves open Outlet valves closed Blood volume in ventricle at end of diastole = end diastolic volume (EDV) Cardiac pump cycle: diastole
Emptying/ejection stage Ventricular contraction Blood pumped from ventricles to arteries AV valves closed Outlet valves open Blood volume in ventricle at end of systole = end systolic volume (ESV) Cardiac pump cycle: systole
The volume of blood ejected from the heart in one pump cycle is called the stroke volume Cardiac pump cycle: stroke volume
Cardiac physiology • Heart rate = number of diastolic/systolic phases occurring per unit time • Cardiac output = bulk flow of blood generated by pumping action of heart CO (mL/min) = HR (beats/min) x SV (mL/beat)
Autoregulation: VR = CO (The stroke volume will be altered such that the heart pumps out the same volume of blood it receives during diastole) Cardiac physiology • Venous return (VR) = variable flow of blood entering the heart • Variable to compensate for physiological state • i.e. VR during exercise
Important cardiac features: • Sinoatrial node (SA node) • Atrioventricular node (AV node) • Bundle of His • Purkinje fibers Functional anatomy: conduction • The heart is excited by the coordinated contraction of cardiac muscle cells • Cells act as syncitium due to gap junctions • Impulse initiating concuction = action potential
Node at junction of superior vena cava and R atrium Function = spontaneously generates APs Intrinsic cardiac pacemaker Conduction: SA node
Only forward conduction! Conduction: AV node • Located behind tricuspid valve • Function: conduction delay (critical for cardiac pumping) • AP propagation: • Slow (delay between atria + ventricles) • Few gap junctions • Less negative RMP
Conduction: bundle of His • Muscle fibers within interventricular septum - splits into 2 branches • Function: conduct AP impulse throughout the R + L ventricles • Rapid conduction occurs within msec of receiving the impulse
Conduction: purkinje fibers • Fibers spread throughout endocardial surface of ventricular muscle • Function: to conduct AP impulse to the actual ventricular muscle mass • Very rapid conduction transmission
Cardiac muscle functions as a syncitium, with fibers separated by intercalated disks Depolarization spreads over entire heart Followed by contraction of entire myocardium So the heart functionally behaves as one cell! Finally, the recruitment of cells to actively participate in contraction is not a regulatory event that occurs in the heart Cardiac action potentials
Cardiac ion channels Resting K+ channels Fast Na channels Outward K+ channels Slow Ca2+ channels Delayed K+ channels Cardiac action potentials • Two functional syncitiums: Atrial & Ventricular • APs are conducted between these two (from atrial ventricular syncitium) via the AV bundle • Spread of AP between each cardiac cell: • Occurs within intercalated disks • High in gap junctions (high electrical conductance)
Cardiac action potentials • Frequent spontaneous depolarizations occur in the SA node • SA node cells control the heart rate by emitting new APs before the AV node or purkinje fibers • Depolarization spreads through heart, developing unique APs at each site
1 2 3 0 4 Ventricular action potentials • Phase 0: depolarization • Phase 1: early repolarization • Phase 2: Plateau • Phase 3: terminal repolarization • Phase 4: RMP
1 2 3 0 4 Ventricular action potentials • Phase 0: depolarization • Spontaneous depolarization • Threshold potential reached • Fast voltage-gated Na+ channels open • Na+ channels inactivate and don’t contribute to phases 1-4
1 2 3 0 4 Ventricular action potentials • Phase 1: early repolarization • Due to transient K+ channels • Open rapidly for K+efflux • These actually inactivate very soon after they are activated
1 2 3 0 4 Ventricular action potentials • Phase 2: plateau • Delayed K+ channels open • K+ efflux will repolarize • At the same time, Ca2+ channels are activated • Ca2+ entry will depolarize • K+/Ca2+ movement works against each other to create plateau
1 2 3 0 4 Ventricular action potentials • Phase 3: terminal reploarization • Ca2+ channels inactivate • K+ channels still open! • Delayed K+ channels open fully and are at peak activity • Massive K+ efflux with no counteraction by Ca2+
1 2 3 0 4 Ventricular action potentials • Phase 4: resting potential • Delayed K+ channels close • Potential now generated by resting K+ channels • Sets cardiac cells back to resting membrane potential to prepare for another AP
Action potentials in the AV node • Similar to SA node • Conduction is slow! Nodal action potentials • Action potentials in the SA node • Automaticity (pacemaker cells) • Primarily phase 0 • Phases 1 + 2 are absent! • Slow voltage-gated Ca+ channels
Significance of cardiac APs • Normal rhythmic contractions of heart occur due to spontaneous SA activity • The heart rate (interval between beats) is determined by how long it takes cells to reach threshold level and fire an AP • Neural influences from autonomic nervous system affect the rate of depolarization
Cardiac Physiology Pressure-volume relationships
Terms • Pre-load • load on the muscle prior to contraction • Muscle length determined by EDV • Afterload = Load muscle sees during contraction • Total load = pre-load + afterload • Contractility • vigor of contraction forcefullness • Depends on degree of Ca2+ activation in cardiac muscle
SV = EDV – ESV Changing muscle load • Increasing pre-load • Increases the degree of shortening cardiac muscle is capable of • Increases the SV! • Increasing afterload • Negatively affects cardiac muscle shortening • Decreases the SV! • Afterload increases during pathophysiologic states such as hypertension or valve obstruction
T = P r Law of LaPlace • Defines the pressure-volume relationship of the working heart • Cardiac muscle fibers surround the ventricular wall such that changes in the fiber length is proportional to changes in the ventricular radius • Ventricular wall tension (T) depends on the intraventricular pressure (P) and radius (r)
Law of La Place Situation A: • Beginning of diastole • Prior to filling • T = P r Situation B: • End of diastole (EDP) • Pre-load (after filling) • 2T = P 2r • Enlarged radius = greater tension!
Law of La Place Situation C: • Beginning of contraction • Prior to ejection • 50T = 25P 2r • pressure from filling Situation D: • End of systole (ESP) • 50T = 50P r • radius but still lots of pressure
Pressure volume loops • After diastolic filling = EDV develops a small pressure (EDP), which is the pre-load • After filling ceases, Pleft ventricle > Pleft atrium • Mitral valve closes
Pressure volume loops • Mitral valve closes, but blood remains in ventricle so ventricular pressure keeps rising • During isovolumetric contraction, Pventricle > Paorta
Pressure volume loops • When Pventricle < Paorta the aortic valve closes • Relaxation begins and pressure within the ventricle drops • The cycle starts over with filling when Pventricle < Patrium
pre-load = SV afterload = SV Altered P-V loops
Altered P-V loops contractility = SV
Venous Return • VR = volume of blood brought back to heart • Through autoregulation, the heart adapts to any influences on blood volume such that VR = CO The Frank-Starling law of the heart • Output values for R + L ventricles are maintained in balance