Download
1 / 37
380 likes | 406 Views
This presentation discusses the rising concern of Vitamin D deficiency, optimal testing and treatment strategies, and clinical implications. It covers sources of Vitamin D, epidemic proportions, related diseases like osteomalacia, and case studies for practical application in patient care.

E N D
Vitamin D for the GP Rod Hughes Rheumatology ASPH 6th Oct 2011
Surrey data • 50% of the population is Vitamin D deficient • 150,000 ‘potential’ cases • Exponential rise in ordering of Vitamin D testing • Cost per test - £2.90 ASPH
The size of the problem • No-one is sure how to treat • No-one is sure when to treat • No-one is sure who to treat • No-one is sure how long you treat for
Vitamin D – clinical issues • Should we be restricting access to testing? • Should we be testing everyone? • When to test • What time of year • When to treat • What with and for how long • How to reassure the worried well
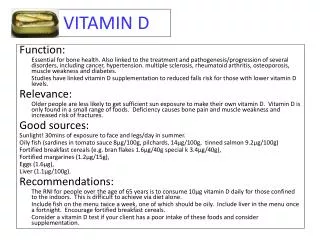
Sources of Vitamin D • Vitamin D2 – ergocalciferol – synthesised by plants • Vitamin D3 – cholecalciferol the analyte – colecalciferol the drug – from UVB effect on skin of invertebrates – naturally in fish • Vitamin D measurement = 25 hydroxy Vit D – raised by both Vit D2 and D3
Sources of Vitamin D • 2-3 exposures of 20-30 mins sunlight per week should provide enough Vit D for adults in the UK • Sun exposure due to latitude in the UK insufficient to provide needs Oct through to April • Diet – oily fish, egg yolks, light exposed mushrooms and liver + fortified products
Some facts • Half the world’s population is Vit D deficient Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357:266-81 • The Institute of Medicine (IOM)Nov 2010 recommends increasing the daily vitamin D intake for children and adults to 600 IU per day for people ages 1 to 70, and 800 IU for people over age 70. • A combined analysis of multiple studies found that taking 700 to 1,000 IU of vitamin D per day lowered the risk of falls by 19 percent, but taking 200 to 600 IU per day did not offer any such protection. Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. 2009; 339:b3692. • Low vitamin D levels might somehow increase colon cancer risk Garland CF, Garland FC. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int J Epidemiol. 1980; 9:227-31.
Osteomalacia Impaired mineralisation phase of remodelling • Spinal bone pain • Pelvic pain • Leg pain • Muscle weakness • Hypocalaemia • Pelvic flattening • Low trauma fractures • Bone softening and bending of bones
Clinical presentation • Insidious onset • Lumbar pain • Lordosis and pelvic flattening • Waddling gait • Low trauma fractures • Bone sensitivity on pressure • Easy fatiguability
Assays • Assay of serum 25-hydroxy Vit D by measuring 25-hydroxy D3 or total 25 hydroxy D2 and D3 <25 nmol/L – severely deficient – below this level PTH starts to rise and bone turnover increases 25-50 nmol/L – insufficient 50-75 nmol/L - adequate >75 nmol/L – normal and replete Highest levels at the end of summer and lowest in the early Spring
Case 1 • 34 year old doctor 28 weeks pregnant 1st pregnancy • Tired – aching – feels unwell • Sees her GP and asks for Vitamin D levels • Measured 2.07.2011 37nmol/L • Wants to be treated as she feels that her risks for foetal abnormality are increased
Case 1 Management advice • What would you tell her? • What treatment would you give? • What follow up would you give?
Case 2 • 47 year old asian lady presents with proximal myalgia and leg pain • Vitamin D levels June 2011 – 6 nmol/L • No clear cause for deficiency • X rays suggest Looser’s zones tibia bilaterally • Seen at the request of the GP in Rheumatology
Case 2 – Management advice • What would you treat her with? Specific product Dose Duration • What follow up instructions would you give
Case 3 • 54 year old lady with ulcerative colitis • Vitamin D levels via GP 18nmol/L • Feels tired • Joints and muscles ache
Case 3 – management advice • What would you treat her with? Product Dose Duration Route
Who should you test? Features of symptomatic deficiency • Insidious-onset widespread bone pain and tenderness • Proximal muscle weakness • Swelling and tenderness at pseudo-fracture sites • Fractures at osteoporotic sites • Myalgia with raised CPK
Predisposing features • Black and ethnic minorities with dark skin • Elderly patients in residential care and housebound • Intestinal malabsorption • Wearing of a veil or habitual sunscreen • Vegan/ vegetarian • Liver or renal disease • Anti-convulsants / cholestyramine / rifampicin / steroids / anti- retrovirals
Pregnancy • Non-evidence based advice • Pregnant women and women with a baby under 1 yr old and children from six months to age 4 are entitled to free vitamins under Healthy Start programme • Treat severe deficiency in pregnancy to avoid foetal risk
Assessing Vit D status • Serum calcium • PTH (unstable – on site phlebotomy) • Alkaline Phosphatase • Phosphate • Renal function • Liver function • FBC (exclude malabsorption)
Treatment • Colecalciferol (D3) is the preferred form of treatment • Colecalciferol may raise Vit D levels more effectively than ergocalciferol as it binds better to liver enzymes, plasma Vit D binding protein and vitamin D receptors • Some assays only measure metabolites of colecalciferol
What to use? Insufficient • 25-50 nmol/L – oral supplementation of 1000 -2000 units of colecalciferol for 12 weeks • Preferred product is Lambert’s Vit D3 tablets 1000 units • As a fat soluble vitamin D tablets should be taken with food to enhance absorption • Test Vit D after treatment – 3 months later
What to use? Maintenance after treatment 800 – 1000 units daily sometimes for life Adcal D3 (calcium carbonate 1.5g & colecalciferol 400units) one tablet twice daily
Alfacalcidol • 1 – alpha hydroxy colecalciferol • With kidney failure or after parathyroidectomy • 0.25 microgm or 1 microgm capsules • Dose – initial 1 – 3 microgm daily to achieve calcium normality then maintain at 0.25 – 1 microgm daily • Itching / urticaria / hypercalcaemia / kidney stones
Calcitriol (rocaltrol) • 1, 25 dihydroxy colecalciferol • Greater chance of inducing hyper calcaemia • Some data in osteoporosis management • Use with dialysis • Start at 0.25 microgm daily and titrate upwards to 0.5 – 1.0 microgm daily
Case 1 • Reassure • 80% pregnant women have Vit D levels below 75 nmol/L • Suggest supplementation with adcal D3 2 tablets daily • Repeat Vit D 3 months after pregnancy
Case 2 • Preferred treatment Lamberts Vit D3 600iu daily for 1 month • Repeat Vit D levels • Start maintenance supplementation as adcal D3 for life
Case 3 • IM Vit D3 300,000iu 2 x 3 months apart • Repeat Vit D assay • Repeat treatment?
Vitamin D guidelines • Guidance on testing and results interpretation • Help with treatment choice and availability • Avoidance of expensive and sub optimal treatments • Standardise replacement and testing across primary and secondary care