Download
1 / 61
610 likes | 972 Views
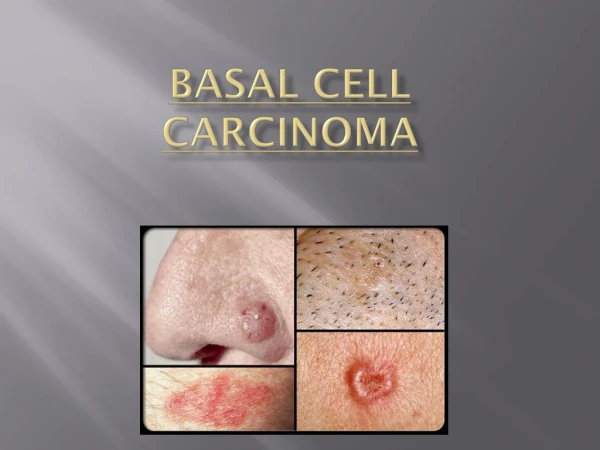
Basal Cell Carcinoma. Presented by: Bill V. Way, D.O. AOCD Board Certified Dermatologist Residency in US Army at Walter Reed Consultant for Charlton Methodist Hosp for past 19 years. Epidemiology and Etiology. Incidence US 500-1000 per 100,000 >400,000 new patients annually

E N D
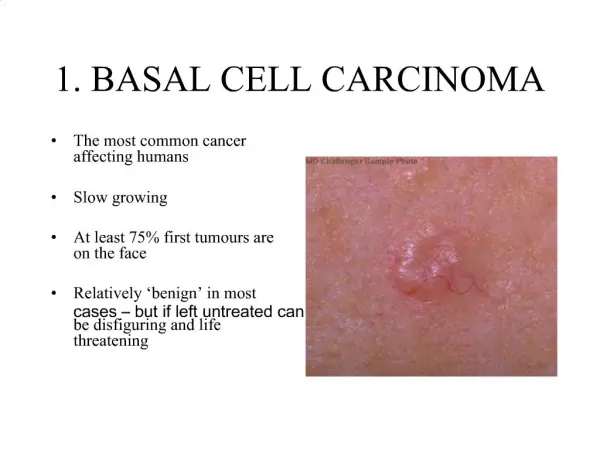
Basal Cell Carcinoma • Presented by: • Bill V. Way, D.O. • AOCD Board Certified Dermatologist • Residency in US Army at Walter Reed • Consultant for Charlton Methodist Hosp for past 19 years
Epidemiology and Etiology • Incidence US 500-1000 per 100,000 • >400,000 new patients annually • Age usually over age 40 • Sex Males >Females • Race rare in brown and black skinned pt
Diagnosis • High index of suspicion • Onset • Prior treatment
Types of BCC • Supeficial BCC • Nodular BCC • Pigmented BCC • Cystic BCC • Sclerosing or Morpheaform BCC • Recurrent BCC
Biopsy • Biopsy: Shave, Punch,Excision • Specimen to reliable dermatopathologist or pathologist
What to Biopsy • Select a good representation of the lesion for biopsy • If small lesion, biopsy the entire lesion • Final treatment code is dependent on actual size of lesion at time of biopsy • Get exact measurements of lesion, digital photo if possible
When should you do a biopsy? • If you are unsure of diagnosis of lesion and have in the differential a skin cancer, basal cell carcinoma, squamous cell carcinoma or melanoma, then do a biopsy • List your differential in the order which you think the lesion is. Learn from your errors.
Methods of Biopsy • Shave Biopsy: easiest and fastest • Punch Biopsy: depth of lesion • Excisional Biopsy: > time, > expense, complete removal of tumor • Incisional Biopsy: partial removal of tumor, >time, > expense
Shave Biopsy • Xylocaine 2% with epi • 1cc tuberculin syringe, 30g needle • Non-sterile gloves • #15 sterile blade Bard Parker • Specimen bottle, labeled correctly • Drysol solution • Bacitracin Ointment, Bandaid
Punch Biopsy • Xylocaine 2% with epi • 1cc tuberculin syringe, 30g needle • Sterile gloves • Punch : 2mm, 3mm, 4mm, 6mm • Minor surgery tray, suture size for area • Specimen bottle labeled correctly • Bacitracin Ointment and bandaid
Excision or Incisional Biopsy • Xylocaine 2% with epi • 3-5cc syringe, 30g needle, sterile gloves • #15 or #11 sterile blade, surgery tray • Suture for area, absorbable, non-absorbable • Specimen bottle labeled correctly • Bacitracin Ointment and sterile dressing
Treatment of BCC • Electrodesiccation and curettage • Excision • Cryosurgery • Moh’s Surgery • Radiation • 5-Fluorouracil • Aldara (Imiquimod)
Electrodesiccation & Curettage • Hyfrecator • Curettes: 2mm, 3mm, 4mm • EDC times 3 • Expect scar formation • 85-90% cure rate • Check for Pacemaker, Defribralator
Excision • Adequate outline of tumor margin • Adequate margins 3-5mm • Surgery Tray, Hyfrecator • Suture: absorbable, non-absorbable • Tag tip, specimen labeled correctly • Pressure dressing, antibiotic ointment
Cryosurgery Used only for superficial and small nodular BCC Not indicated for deeper BCC High morbidity, very painful
Moh’s Surgery • Can be used on all BCC • Difficult lesions: sclerosing or recurrent, poorly defined borders, tumors of nose, eyelids • Recurrent lesions • Lesions over 25mm dia • 98% cure rate • Expensive, > time • Few Moh’s Surgeons, Dermatologist