Download
1 / 1
10 likes | 140 Views
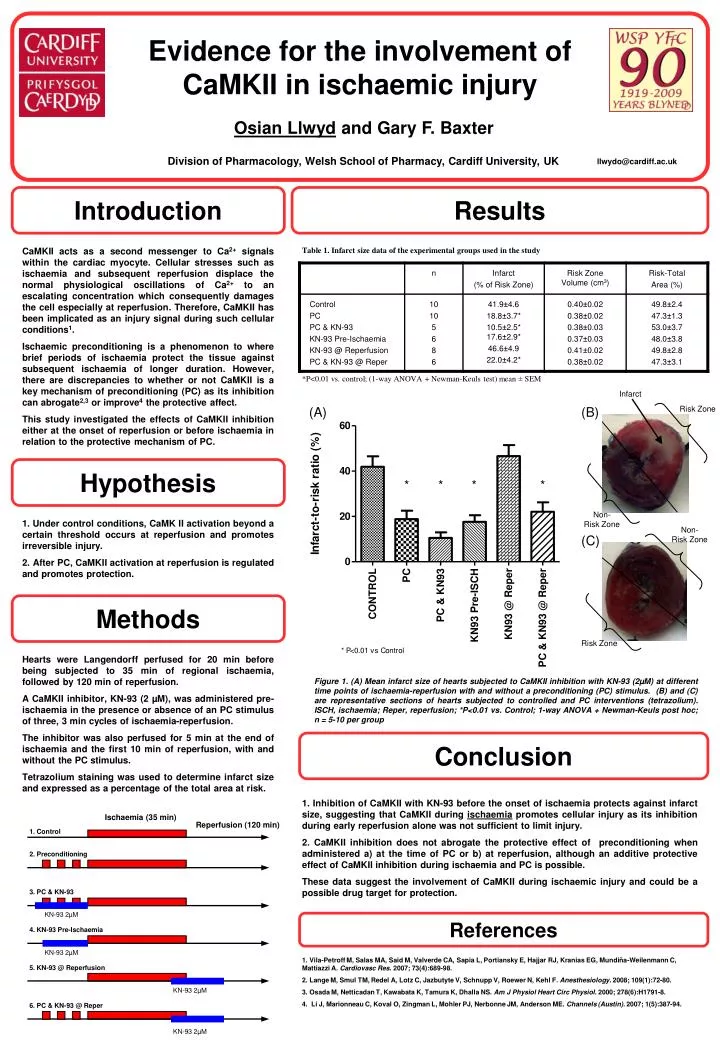
Evidence for the involvement of CaMKII in ischaemic injury. Osian Llwyd and Gary F. Baxter Division of Pharmacology, Welsh School of Pharmacy, Cardiff University, UK. llwydo@cardiff.ac.uk. Introduction. Results.

E N D
Evidence for the involvement of CaMKII in ischaemic injury Osian Llwyd and Gary F. BaxterDivision of Pharmacology, WelshSchool of Pharmacy, Cardiff University, UK llwydo@cardiff.ac.uk Introduction Results CaMKII acts as a second messenger to Ca2+ signals within the cardiac myocyte. Cellular stresses such as ischaemia and subsequent reperfusion displace the normal physiological oscillations of Ca2+ to an escalating concentration which consequently damages the cell especially at reperfusion. Therefore, CaMKII has been implicated as an injury signal during such cellular conditions1. Ischaemic preconditioning is a phenomenon to where brief periods of ischaemia protect the tissue against subsequent ischaemia of longer duration. However, there are discrepancies to whether or not CaMKII is a key mechanism of preconditioning (PC) as its inhibition can abrogate2,3 or improve4 the protective affect. This study investigated the effects of CaMKII inhibition either at the onset of reperfusion or before ischaemia in relation to the protective mechanism of PC. Table 1. Infarct size data of the experimental groups used in the study *P<0.01 vs. control; (1-way ANOVA + Newman-Keuls test) mean ± SEM Infarct (A) (B) Risk Zone Hypothesis Non- Risk Zone 1. Under control conditions, CaMK II activation beyond a certain threshold occurs at reperfusion and promotes irreversible injury. 2. After PC, CaMKII activation at reperfusion is regulated and promotes protection. Non- Risk Zone (C) Methods Risk Zone Hearts were Langendorff perfused for 20 min before being subjected to 35 min of regional ischaemia, followed by 120 min of reperfusion. A CaMKII inhibitor, KN-93 (2 µM), was administered pre-ischaemia in the presence or absence of an PC stimulus of three, 3 min cycles of ischaemia-reperfusion. The inhibitor was also perfused for 5 min at the end of ischaemia and the first 10 min of reperfusion, with and without the PC stimulus. Tetrazolium staining was used to determine infarct size and expressed as a percentage of the total area at risk. Figure 1. (A) Mean infarct size of hearts subjected to CaMKII inhibition with KN-93 (2µM) at different time points of ischaemia-reperfusion with and without a preconditioning (PC) stimulus. (B) and (C) are representative sections of hearts subjected to controlled and PC interventions (tetrazolium). ISCH, ischaemia; Reper, reperfusion; *P<0.01 vs. Control; 1-way ANOVA + Newman-Keuls post hoc; n = 5-10 per group Conclusion 1. Inhibition of CaMKII with KN-93 before the onset of ischaemia protects against infarct size, suggesting that CaMKII during ischaemia promotes cellular injury as its inhibition during early reperfusion alone was not sufficient to limit injury. 2. CaMKII inhibition does not abrogate the protective effect of preconditioning when administered a) at the time of PC or b) at reperfusion, although an additive protective effect of CaMKII inhibition during ischaemia and PC is possible. These data suggest the involvement of CaMKII during ischaemic injury and could be a possible drug target for protection. Ischaemia (35 min) Reperfusion (120 min) 1. Control 2. Preconditioning 3. PC & KN-93 KN-93 2µM References 4. KN-93 Pre-Ischaemia KN-93 2µM 1. Vila-Petroff M, Salas MA, Said M, Valverde CA, Sapia L, Portiansky E, Hajjar RJ, Kranias EG, Mundiña-Weilenmann C, Mattiazzi A. Cardiovasc Res. 2007; 73(4):689-98. 2. Lange M, Smul TM, Redel A, Lotz C, Jazbutyte V, Schnupp V, Roewer N, Kehl F. Anesthesiology. 2008; 109(1):72-80. 3. Osada M, Netticadan T, Kawabata K, Tamura K, Dhalla NS. Am J Physiol Heart Circ Physiol. 2000; 278(6):H1791-8. 4. Li J, Marionneau C, Koval O, Zingman L, Mohler PJ, Nerbonne JM, Anderson ME. Channels (Austin). 2007; 1(5):387-94. 5. KN-93 @ Reperfusion KN-93 2µM 6. PC & KN-93 @ Reper KN-93 2µM