Download
1 / 35
350 likes | 360 Views
Learn about the features, epidemiology, and clinical impact of influenza in pregnant women. Understand the potential risks, symptoms, and complications associated with flu during pregnancy. Discover how the immune system changes during pregnancy and how to manage influenza effectively.

E N D
Influenzaclinical featuresepidemiologydd.SonbolTaramian MDinf.dis.departmentGUMS
pregnant women, children < 59 mths,the elderly, chronic medical conditions(chronic cardiac, pulmonary, renal, metabolic, neurodevelopmental, liver or hematologic dis.) IC:(HIV/AIDS, chemotherapy or steroids, or malignancy)HCW
Changes in immune system, heart, and lungs during pregnancy (and up to 2 wks postpartum) more prone to severe illness from flu, including illness resulting in hospitalization
changes include :elevation of diaphragm to accommodate the uterus, increased respiratory rate, increased intra‐abdominal pressure, decreased chest compliance,and as a consequence,increased risk of aspiration
The pathophysiologic mechanisms underlying increased flu risk to pregnant women and their fetuses are unclear
Replication of flu v. is significantly higher in peripheral blood mononuclear cells (PBMCs) incubated with 3rd trimester serum
rapidtransmissionin crowded areas (schools / nursing homes)coughs or sneezes, in closeproximityby contaminated hands
Adults spread from 1 d. before symptoms to5 d. afterChildren and IC, longer
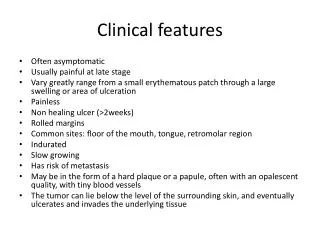
mild to severe illnessfromasymptomatic tomild, uncomplicated tosevere, complicated illness
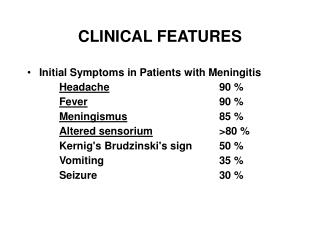
typical symptoms sudden onset of:high fevermuscle achesheadachechillsfatigueloss of appetitesore throatIn some,especially children, nausea, vomiting and diarrhea
pneumoniaa serious complication from flu v. infaloneor co-inf with bac.
Other possible serious complicationstriggered by flu :myocarditis,encephalitis ormyositis, rhabdomyolysis, and multi-organ failure
most , recover in 7 - 10 d.,severe illness can occurv. can triggeran extreme inflammatory response and lead to sepsis
Difficulty breathing orshortness of breathPain or pressure in the chest or abd.Sudden dizzinessConfusionSevere or persistent vomiting
Flu-like symptoms improve but then return withfever and worse cough
Almost all of flu v. examined this season are still similar to the cell-grown vaccine reference v.( not significant Agicdrift)
How commonly mismatch occurs between flu vaccine strains and circulating flu v.?
17 years' of data ,close match only 11% - 21% of time1996 - 2012, 17-yr period divided into 34 flu seasons—winter and summer for each yr.:Northern Hemisphere vaccine strains :closely matched with circulating strains for 7 (20.6%) of 34 seasons for H3N2 and 5 (14.7%) of 34 seasons for flu B. For the Southern Hemisphere vaccine, rates were 14.7% for H3N2 and 11.1% for flu B.Strain drift among seasons: 41.2% for H3N2 and 35.3% for influenza B
In recent yrs multiple novel flu A strains have emerged in humans
MostzoonoticAIVs and swine flu variants typically cause mild inf. in humans however severe illness and fatalities are associated with zoonotic H5N6, H10N8, H7N9 and H5N1 serotypes, and H1N1 1918 Spanish flu.
changing landscape of avian flu globally indicates a need to reassess the risk of a pandemic flu outbreak of zoonotic origin
an increase in emergence of AIVs infecting humans in the last decade (i) improvements in zoonotic AIV case ascertainment,
which could be explained by an increase in AIV circulation and diversity in poultry populations, growths in the poultry industry
not any reports of AIV emergence in humans in low-income, developing countries – this may also be due to case ascertainment bias. Developing countries are both unable to support high levels of active AIV surveillance (in both human and animal sectors), and highly regulated agricultural systems with the ability to enforce dis. control regulations
Avian flu has the highest case-fatality rate among 10-39 yrs. Unlike seasonal flu, (very young and very old individuals),young adults a large proportion of avian flu cases50%,<20 yrs. 40%,aged 20-40 yrsIn Egypt, avian flu ,a relatively low mortality rate, associated with a high rate of inf. in young children (< 10 y); as of May 2009, the mortality rate in this subpopulation has been zeroThe significance and reproducibility of these findings remains to be seen
Infectious diseases causing ILI: malaria, acute HIV/AIDS inf., hepatitis C, Q fever,dengue fever,pneumonia, Pharmaceutical drugs :biologics such as IFN and monoclonal Abs, CSFsChemotherapeutic agentsbisphosphonates, caspofungin, and levamisoleinfluenza vaccine or other vac., opioid withdrawal in addicts
rhinoviruses,coronaviruses, human respiratory syncytial virus, adenoviruses,human parainfluenza v. Less common causes bacegLegionella, Chlamydia pneumoniae, Mycoplasmapneumoniae, and Streptococcus pneumoniae. RSV