Download
1 / 28
280 likes | 443 Views
70 yr old with lethargy and presyncope. Type II AV block – Mobitz II. Same patient few minutes later. Type II block – Wenkebach/Mobitz I . Same patient yet again…. Complete heart block – Third degree block. 70 yr old with lethargy and syncope.

E N D
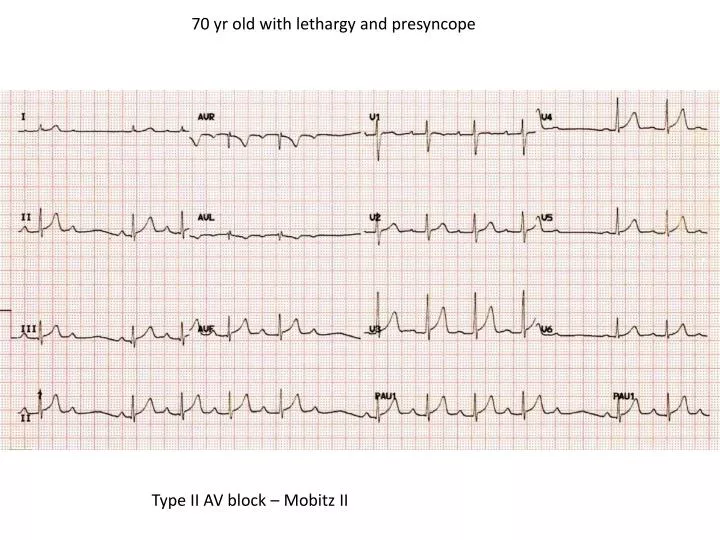
70 yr old with lethargy and presyncope Type II AV block – Mobitz II
Same patient few minutes later Type II block – Wenkebach/Mobitz I
Same patient yet again… Complete heart block – Third degree block
70 yr old with lethargy and syncope Trifascicular block – 1st degree HB, RBBB and LAD (L anterior hemiblock)
50 yr old with palpitations Capture beats Fusion beat Monomorphic VT
You don’t want this for your patient Ventricular Fibrillation
30 yr old male with syncope Brugada Syndrome
Brugada Syndrome • ECG Findings • Three types • ST elevation v1 – v3 > 2mm • Complete or incomplete RBBB • T-wave α types • 1. Inverted • 2. Biphasic • 3. Upright
Brugada – Why do we care? • Predisposition to polymorphic ventricular tachycardia • Identification and treatment with AICD may prevent a young sudden cardiac death
25 year old with syncope on exercising Arrthymogenic RV cardiomyopathy/dysplasia - inverted T waves in leads V1 through V5. Arrowheads point to late RV activation, called an epsilon wave
When to refer cardiac syncope to ED • All 2nd degree and 3rd degree heart blocks • All trifascicular blocks • All rapid AF >120 • All SVTs in not terminated by Valsalva manouvre • “funny looking” ST/T segments – discuss/fax • Asymptomatic patients with WPW, ST changes can be referred to cardiology OPA
Important contact details for Northern Hospital Nov 2013 Clinical ED Consultant – 8405 2610/8405 8610 ED Fax – 8405 8633 EMET/General enquiries – 8405 8013 (Kim Tarzia ED secretary) EMET queries to Dr Cynthia Lim, Dr Peter Jordan, Dr Megan Robb ED Director – Dr ShyamanMenon EMET presentations : www.nhedventures.com Adult Outpatients – 8405 8850/8405 8335 Fax – 8405 8761 Cardiology – 8405 8859 Fax – 8405 8405 (currently 3 month wait for Chest pain clinic) Paediatric/Paed Surgery OPA – 8405 8417 Fax – 8405 8449 (current 4-6 week)(apmt sent 1 week) Paediatric Surg Fax – 8405 8449 (within a week)
www.nhedventures.com Click on EMET on left to access presentations provided. Registrar education sessions and interesting education links
70 yr old with lethargy and presyncope Type II AV block – Mobitz II
Same patient few minutes later Type II block – Wenkebach/Mobitz I
Same patient yet again… Complete heart block – Third degree block
70 yr old with lethargy and syncope Trifascicular block – 1st degree HB, RBBB and LAD (L anterior hemiblock)
50 yr old with palpitations Capture beats Fusion beat Monomorphic VT
You don’t want this for your patient Ventricular Fibrillation
30 yr old male with syncope Brugada Syndrome
Brugada Syndrome • ECG Findings • Three types • ST elevation v1 – v3 > 2mm • Complete or incomplete RBBB • T-wave α types • 1. Inverted • 2. Biphasic • 3. Upright
Brugada – Why do we care? • Predisposition to polymorphic ventricular tachycardia • Identification and treatment with AICD may prevent a young sudden cardiac death
25 year old with syncope on exercising Arrthymogenic RV cardiomyopathy/dysplasia - inverted T waves in leads V1 through V5. Arrowheads point to late RV activation, called an epsilon wave
When to refer cardiac syncope to ED • All 2nd degree and 3rd degree heart blocks • All trifascicular blocks • All rapid AF >120 • All SVTs in not terminated by Valsalva manouvre • “funny looking” ST/T segments – discuss/fax • Asymptomatic patients with WPW, ST changes can be referred to cardiology OPA
Important contact details for Northern Hospital Nov 2013 Clinical ED Consultant – 8405 2610/8405 8610 ED Fax – 8405 8633 EMET/General enquiries – 8405 8013 (Kim Tarzia ED secretary) EMET queries to Dr Cynthia Lim, Dr Peter Jordan, Dr Megan Robb ED Director – Dr ShyamanMenon EMET presentations : www.nhedventures.com Adult Outpatients – 8405 8850/8405 8335 Fax – 8405 8761 Cardiology – 8405 8859 Fax – 8405 8405 (currently 3 month wait for Chest pain clinic) Paediatric/Paed Surgery OPA – 8405 8417 Fax – 8405 8449 (current 4-6 week)(apmt sent 1 week) Paediatric Surg Fax – 8405 8449 (within a week)
www.nhedventures.com Click on EMET on left to access presentations provided. Registrar education sessions and interesting education links