Download

1 / 32
320 likes | 493 Views
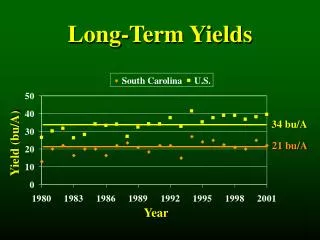
Martin Samuels University Hospital of North Staffordshire. INITIATING long term ventilation. Initiating Long Term Ventilation. why? when ? how ? where? what with?. Conditions Receiving LTV. Failure of resp pacemaker nerve conduction muscle contraction airway patency gas exchange

E N D
Martin Samuels University Hospital of North Staffordshire INITIATINGlong term ventilation
Initiating Long Term Ventilation • why? • when ? • how ? • where? • what with?
Conditions Receiving LTV Failure of • resp pacemaker • nerve conduction • muscle contraction • airway patency • gas exchange • combination CCHS infection, trauma DMD, SMA severe TBM CLD of prem, CF neurodisability, obesity
When to Initiate LTV at presentation: • birth • after trauma • after infection • with acute respiratory illness eg CCHS, CLD operative, RTC myelitis myopathy, CF
When to Initiate LTV Conditions Presenting with Progressive Respiratory Failure • myopathy • neurodisability • obesity
Neuromuscular Conditions with Ventilatory Failure Hereditary muscular dystrophies myopathies spinal muscular atrophy hereditary sensory n myotonic dystrophy Work with colleagues in muscle disorders Acquired polio Guillain-Barre polymyositis myasthenia gravis
Survival in Type I SMAwithout ventilatory support Dubowitz et al (from JTSMA)
When to Initiate LTV • myotonic dystrophy • spinal muscular atrophy II • neuropathy • nemaline rod myopathy
Duchene MD • median fall FVC 0.18L/y • median survival 3.1y • 5y survival 8% • Phillips et al, 2001
Recognition of Respiratory Failure • early recognition • symptoms • LFT’s • SaO2 & CO2 monitoring • awareness of treatment options
Monitoring Equipment SenTec SaO2 & tcPCO2 Capnocheck SaO2 & ET-CO2
Case B Apr 2002 - 14y - DMD • care plan for terminal care: no CPR, intubation or ‘active’ intervention • referral for respiratory assessment May 2002 • Found unresponsive at home… A&E • CO2 found to be 11.6 kPa
Case B May 2002 • admitted for sleep study • would not wake: pCO2 27 pH 7.0 • bagged: pCO2 19 • nPPV no better – agreed not for ETT • family counselled
Case B • Intubated for 3/7 • Prednisolone • Extubated • Discharged • nPPV • Cough Assist
Development of Respiratory Failure Insidious onset patients appear normal when awake REM sleep all sleep awake
Presentation of Nocturnal Hypoventilation • Nocturnal arousals • Behavioural and cognitive problems • Daytime drowsiness / poor concentration • Failure to thrive • Morning headaches • Recurrent / severe LRTI’s • Cor pulmonale (late)
Assessment in DMD Fall in VC • hypoxaemic-apnoeic episodes • rise in CO2 & fall in SpO2 • in REM sleep first • lastly, during day Overnight record of SaO2 & CO2 • ? age 10 – 12y • ? VC <30%, 50%, 60% …
SaO2 Whole night: 8h Heart rate Transcutaneous pCO2
Mail questionnaire: Canadian physicians • Response rate 45/60 • 25% do not discuss mech vent with all patients & families • Most frequently cited reason for advising against / withholding ventilation was poor quality of life (52.6%)
When to Initiate LTV • progressive respiratory failure • quality of life reduced: • symptoms • repeat / severe LRTI • hospitalisation • compliance likely
LTV as part of Palliative Care • improves symptoms • keep out of hospital • ease care by parents • reduce complications • use in overall care plan
RCPCH Guidelines • “No purpose” situation: degree of physical or mental impairment will be so great that it is unreasonable to expect them to bear it • “Unbearable” situation: child and/or family feel that in the face of progressive and irreversible illness further treatment is more than can be borne
How to Initiate LTV • Assessment • Consult • Discuss with family • “Decisions must never be rushed and must always be made by the team with all evidence available.”
Where to Initiate LTV • Hospital v Home • training • troubleshooting • adjustments • PICU v HDU v ward
Initiating LTV – Choosing PPV Device B&D Nippy Breas Vivo Respironics Synchrony Resmed VPAP
Initiating LTV • Face v nasal mask v prongs • Sizing • Humidity • Complications • Monitoring
Complications • Mask intolerance • Skin sores • Dry eyes • Rhinitis • Air swallowing • ? Facial deformity
Other Respiratory Interventions • physiotherapy • immunisation • antibiotics • nutrition • Rx of GORD • in-exsufflator
Summary - Initiating LTV • Why are we initiating this? • Have we consulted / discussed? • How are we going to do it? • Where are we doing this? • What are we going to monitor? • What about discharge?