Download
1 / 32
320 likes | 336 Views
Explore the dynamic landscape of acute heart failure management between current guidelines and patient needs. Delve into the rapid onset symptoms, diagnostic challenges, treatment strategies, and considerations for comorbidities and renal failure.

E N D
IX International Symposium HEART FAILURE & Co. Milano, 18 Aprile 2009 “Re-thinking acute heart failure approach” Acute Heart Failure Management between Current Guidelines and Patient Needs Susanna Sciomer - Francesco Fedele Dept. ofCardiovascular, Respiratory and MorphologicalSciences “Sapienza” UniversityofRome, Italy
+ ESC guidelines 2005
Acute heart failure: a rapid onset or change in the signs and symptoms of HF, resulting in the need for urgent therapy. AHF may be either new HF or worsening of pre-existing chronic HF. Multiple cardiovascular and non-cardiovascular morbidities may precipitate AHF. STROKE VOLUME? General clinical classification Gheorghiade M, Pang PS. JACC 2009; 53:557
Acute Exacerbations Contribute to the Progression of the Disease AHF Functional ability With each event, myocardial injury may contribute to progressive LV dysfunction Worsening signs and symptoms, Neurohormonal and renal abnormalities Occurr soon after discharge CHF CHF High post-discharge event AHF Time Gheorghiade M et al. Am J Cardiol. 2005; 96 (6A)
GUIDELINES AHF between Current Guidelines and Patient Needs… Currently available assessment modalities combined with recent advances in cardiovascular therapies provide present-day opportunities to improve post-discharge outcomes. HF (as a diagnosis at hospital discharge) has tripled over the last 3 decades. This trend will likely continue due to:aging population, improved survival after myocardial infarction, better prevention of sudden cardiac death.
Management of AHF and diagnostic problems Diagnosis is more likely in the presence of multiple typical symptoms and signs (ex. dyspnoea, fatigue, third heart sound, oedema, raised jugular venous pressure.....) The presence of several signs has a good specificity but a low sensibility Need of instrumental objective data to assess the diagnosis Need to exclude other pathologies Gheorghiade M, Pang PS. JACC 2009; 53:557 True typical symptoms?
Two-Minute Assessment of Haemodynamic Profile Forrester’s diagram Cardiac Index 2.2 l/mq 18 mmHg Wedge pressure Pulmonary Edema Normal Hypovolemic Shock Cardiogenic Shock Evidence for Congestion (elevated filling pressures) Orthopnea High Jugular Venous Pressure Increasing S3 Loud P2 Edema Ascites Rales (uncommon) Abdominojugular Reflux Congestion at Rest? No Yes Evidence for Low Perfusion Narrow Pulse Pressure Pulsus Alterations May be Sleepy, Obtunded ACE-inhibitor-Related Symptomatic Hypotension Declining Serum Sodium Level Worsening Renal Function No Warm and Wet Warm and Dry Low Perfusion at Rest? Yes Cold and Dry Cold and Wet Nohria, JAMA 2002; 287: 628
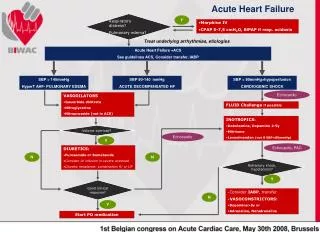
Diagnosis and initial treatment algorithm of AHF ESC guidelines 2008
Non-invasive haemodynamic evaluation (EF, SV, CI, PAPs…) Gheorghiade M, Pang PS. JACC 2009; 53:557
Systemic Peripheral Resistance = Stroke Volume Contractility AHF treatment strategy according to systolic blood pressure ESC guidelines 2008 LV end-Diastolic Volume Preload SystemicPressure Cardiac Output LV end-Systolic Volume Afterload Heart Rate
LV end-diastolic volume - LV end-systolic volume= STROKE VOLUME ???
Inotropic agents Inotropes with vasodilator properties should be reserved for those pts with low-output state (low BP with organ hypoperfusion), who don’t respond to other therapies. CO and SV PCWP • Improves cardiac contractility by binding to Troponin C in cardiomyocytes • Significant vasodilation through ATP-sensitive potassium channels • Mild PDE inhibitory action
Inotropic agents ESC Guidelines 2008 Dobutamine: cl IIa, Level Evidence B PDEIs: cl IIb, Level Evidence B Dopamine: cl IIb, Level Evidence C Levosimendan: cl IIa, Level Evidence B Several inotropic agents are currently available for AHFS; most of them do not appear to be safe and effective; despite significant improvement in the hemodynamic profile, they have potential deleterious effects on:Myocardium (increased myocardial oxygen demand) Blood Pressure (hypotension) Renal Function (impairment) Digoxin iv : cl IIb, Level Evidence C • Increasing cardiac output • Reduction of filling pressure • Slow ventricular rate in rapid AF
GUIDELINES AHF between Current Guidelines and Patient Needs…
AHF Considerations In elderly people comorbidities are the rule. An overlapping is frequent between comorbidities and precipitating factors. NY Heart Failure Consortium, JACC 2004
Comorbidities and precipitating factors of AHF ESC guidelines 2008
The Cardio-RenalSyndrome ESC guidelines 2008 Gheorghiade M, Pang PS. JACC 2009; 53:557
HEART FAILURE & RENAL FAILURETerapheuticalApproach • Evaluation of anaemia and electrolytes • Drug monitoring • Ultrafiltration: -No responsiveness to conventional therapy (moderate-severe RF with creatinine > 2,5- 3 mg/dl) -Emergency treatment in severe acute HF with fluid overload -Long-term treatment in pts who can’t undergo heart transplant
Clinical effects • Reabsorption of systemic and pulmonary oedema • Haemodynamic stability • Hyponatremia correction • Increase of diuresis, natriuresis and responsiveness to diuretics • hormons (NA, PRA, Aldosterone) • Removal of toxins and mediators (citokins, TNF) that impaired myocardial and renal function (?) Costanzo MR, Maya E. et al. JACC 2007
Haemodynamic effects L/min/m2 mmHg b/min Cardiac Index * * Heart rate MAP mmHg mmHg Right Atrial Pressure Wedge Pressure Before UF After UF Overcoming the spatial competition between heart and lungs Courtesy of “CCM”
Ultrafiltration vs. Furosemide in Moderate Heart Failure Body Weight Plasma Renin Activity kg % * * p<0.01 vs. day 0 * * * * * * * * * * * * * * day day UF (n=8; 1710 ml) Agostoni et al. Am J Med 1994 Furosemide (n=8; 248 mg i.v.)
HEART FAILURE AND COPD HEART FAILURE PATIENT CHRONIC PULMONARY DISEASES
Clinical classification of AHF ESC guidelines 2008
EVALUATION of SYSTOLIC RV PERFORMANCE TAPSE Tricuspid Annular Plane Systolic Excursion The level of excursion of the tricuspid valvular plane during systole (TAPSE) corresponds with RV ejection fraction (5 mm ~ 20% RVEF, 10 mm ~ 30% RVEF, 15 mm ~ 40% RVEF, and 20 mm ~ 50% RVEF). Bleeker GB, Heart 2006
RV is fully involved in HF and its function is an important prognostic marker. • Evaluation of PAP and RV function can provide some indipendent predictors of mortality in HF. Evaluation of Pts with HF Functional evaluation of RV = Fundamental !
Goals of treatment in AHF Goals of treatment in CHF • To reduce mortality • To reduce morbidity • Prevention ESC guidelines 2008 Improving post-discharge outcomes is the most important goal in AHFS
The right drug at the right time + apropriate management of comorbidities!!! Multidisciplinary approach ESC guidelines 2008
REVIVE II: Primary Endpoint (n=600) 60 Placebo Levosimendan 30 20 % Patients 10 P=.015 0 Improved Unchanged Worse Packer M, et al. Presented at AHA Scientific Sessions 2005
SURVIVE JAMA, May 2, 2007 – Vol. 297
REVIVE Conclusions SURVIVE Conclusions • Previous ADHF studies focused on single measurements of symptoms or hemodynamic improvement • REVIVE was a positive trial with a Clinical Composite Endpoint that assessed benefit over 5 days • Patient & Physician Global Assessments and Patient Assessment of Dyspnea all support the outcome of the primary endpoint • The safety and mortality profile of levosimendan can be explained in terms of the baseline characteristics (ie, blood pressure) of patients and the mechanism of the drug • The higher Mortality Risk was observed in the Levosimendan low baseline blood pressure cohort • The SURVIVE trial demonstrated no survival difference between Levosimendan and Dobutamine during long-term follow-up despite evidence for an early reduction of plasma BNP level for Levosimendan. • These findings may be related to: - the short duration of treatment in the trial; - a selective effect of Levosimendan in specific subgroups; - the lack of a true difference between the two drugs. • Further studies are needed to distinguish between these possibilities.