Download
1 / 21
230 likes | 711 Views
1. The Surgical Infection Prevention and Surgical Care Improvement Projects National Initiatives to Improve Surgical Care. Dale W. Bratzler, DO, MPH QIOSC Medical Director. Why focus on surgical quality?. ~30 million major operations each year in the US

E N D
1 The Surgical Infection Preventionand Surgical Care Improvement ProjectsNational Initiatives to Improve Surgical Care Dale W. Bratzler, DO, MPH QIOSC Medical Director
Why focus on surgical quality? • ~30 million major operations each year in the US • Despite advances in surgical and anesthesia technique and improvements in perioperative care, variations in outcomes for patients having surgery are well known
Why focus on surgical quality? • Among the most common complications • surgical site infections (SSIs) and postoperative sepsis • cardiovascular complications including myocardial infarction • respiratory complications including postoperative pneumonia and failure to wean • thromboembolic complications
Cost of Complications • Attributable costs • Infectious complications - $1398 • Cardiovascular complications - $7789 • Respiratory complications - $52466 • Thromboembolic complications - $18310 Dimick JB, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531-7.
Surgical Care Improvement ProjectNational Goal 36 To reduce preventable surgical morbidity and mortality by 25% by 2010
American College of Surgeons American Hospital Association American Society of Anesthesiologists Association of peri-Operative Registered Nurses Agency for Healthcare Research and Quality Centers for Medicare & Medicaid Services Centers for Disease Control and Prevention Department of Veteran’s Affairs Institute for Healthcare Improvement Joint Commission on Accreditation of Healthcare Organizations SCIP Steering Committee 37
Surgical Site Infections (SSI) 2 • 2-5% of operated patients will develop SSI • 40 million operations annually in the U.S. • 0.8 - 2 million SSI’s occur annually in the U.S. • SSI increases LOS in hospital • average 7.5 days • Excess cost per SSI: • *$2,734-26,019 (1985, US$) • US national costs: $130-845 million/year *Jarvis, Infect Control HospEpidemiol. 1996;17.
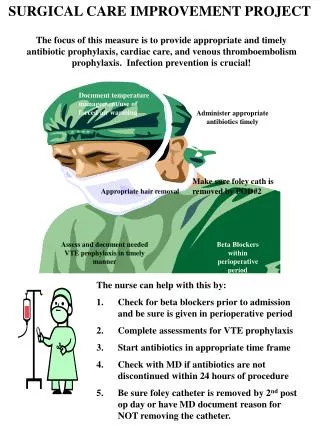
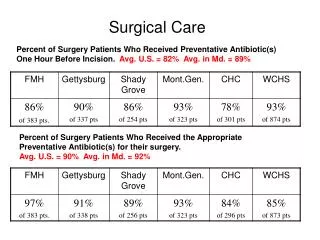
Quality IndicatorsNational Surgical Infection Prevention Project • Proportion of patients who have their antibiotic dose initiated within 1 hour before surgical incision (2 hours for vancomycin or fluoroquinolones) • Proportion of patients who receive prophylactic antibiotics consistent with current recommendations (published guidelines) • Proportion of patients whose prophylactic antibiotics were discontinued within 24 hours of surgery end time (48 hours for cardiac surgery)
Revision to SCIP Inf 2 22 • We will allow for the use of vancomycin for prophylaxis for cardiac, vascular, and orthopedic surgery, if… • There is a physician-documented reason in the medical record • Beta-lactam allergy • We may do some hospital-specific audits of vancomycin use in outlier institutions
Recently Updated Antibiotic Recommendations 25 * For the purposes of national performance measurement a case will pass the antibiotic selection performance measure if vancomycin is used for prophylaxis (in the absence of a documented beta-lactam allergy) if there is physician documentation of the rationale for vancomycin use (effective for July 2006 discharges). Bratzler DW, Hunt DR. Clin Infect Dis. 2006 (in press).
Recently Updated Antibiotic Recommendations (continued) 26 * Ciprofloxacin, levofloxacin, gatifloxacin, or moxifloxacin (effective for July 2006 discharges). † For the purposes of national performance measurement, a case will pass the antibiotic selection indicator if the patient receives oral prophylaxis alone, parenteral prophylaxis alone, or oral prophylaxis combined with parenteral prophylaxis. Bratzler DW, Hunt DR. Clin Infect Dis. 2006 (in press).
Other Points about the Antibiotic Measures • SCIP Inf 2 – May see public reporting on Hospital Compare of July 2006 discharges • SCIP Inf 3 – Any antibiotics given in the first 48 hours after surgery (72 hours for cardiac surgery) are considered “prophylactic” in the absence of a documented infection
Surgical Care Improvement ProjectNew Performance measures - Process 39 • Surgical infection prevention • Glucose control in cardiac surgery patients (< 200 mg/dL) • Blood glucose closest to 0600 on PO day 1 and 2 (surgery end date is PO day 0) • Proper hair removal • No hair removal, clippers, or depilatory • Normothermia in colorectal surgery patients • Temperature between 96.8-100.4° F within the first hour after leaving the OR
Prevention of Cardiac EventsIntroduction 44 • As many as 7 to 8 million Americans that undergo major noncardiac surgery have multiple cardiac risk factors or established coronary artery disease • More than 1 million cardiac events annually • Myocardial ischemia either clinically occult or overt confers a 9 - fold increase in risk of unstable angina, nonfatal myocardial infarction, and cardiac death Schmidt M, et al. Arch Intern Med. 2002;162:63-69. Mangano DT, et al. N Engl J Med. 1996;335:1713-1720. Selzman CH, et al. Arch Surg. 2001;136:286-290.
Surgical Care Improvement ProjectPerformance measure - Process 45 • Perioperative cardiac events • Perioperative beta blockers in patients who are on beta blockers prior to admission “perioperative” is defined as 24 hours prior to incision through discharge from the post-anesthesia care/recovery area
Prevention of Venous ThromboembolismIntroduction 51 • VTE Remains a major health problem • 200,000 new cases annually in US • In addition to the risk of sudden death • 30% of survivors develop recurrent VTE within 10 years • 28% of survivors develop venous stasis syndrome within 20 years • The incidence of VTE is more than 100 times greater for patients who have been hospitalized than among community dwelling • Incidence increases with age Goldhaber SZ. N Engl J Med. 1998;339:93-104. Silverstein MD, et al. Arch Intern Med. 1998;158:585-593. Heit JA, et al. Thromb Haemost. 2001;86:452-463. Heit JA. Clin Geriatr Med. 2001;17:71-92. Heit JA, et al. Mayo Clin Proc. 2001;76:1102-1110.
Surgical Care Improvement ProjectPerformance measures - Process 55 • Prevention of venous thromboembolism • Surgery patients with recommended VTE prophylaxis ordered • Surgery Patients Who Received Appropriate Venous Thromboembolism Prophylaxis Within 24 Hours Prior to Surgery to 24 Hours After Surgery Based on the 2004 ACCP Consensus Recommendations