Download
1 / 34
400 likes | 1.31k Views
Musculoskeletal tb hip joint FIRM III orthopaedic GRANDROUND dr. ondari n . J - ortho ii. 02-05-2013. Tuberculosis is probably as old as mankind. It's continued presence midst us is a sorry tale of missed opportunities and mismanagement by the medical profession. Shanmugasundaram T K.

E N D
Musculoskeletal tbhip jointFIRM III orthopaedic GRANDROUNDdr. ondari n . J - ortho ii 02-05-2013
Tuberculosis is probably as old as mankind. It's continued presence midst us is a sorry tale of missed opportunities and mismanagement by the medical profession Shanmugasundaram T K
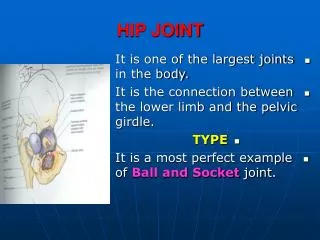
Epidemiology cont. • Bones and joints and affected in ~5% of pts with TB • Commonest is spinal TB in ~50% of cases • Hip – 15% of all osteoarticular TB • Can occur in any age group but is more common in children. • Next common after spinal TB
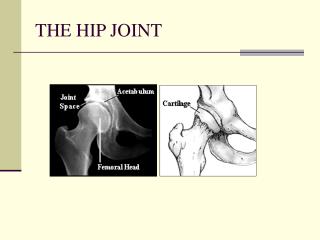
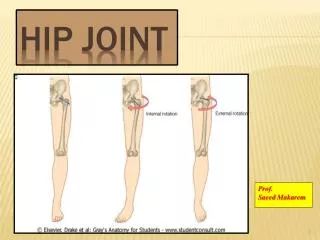
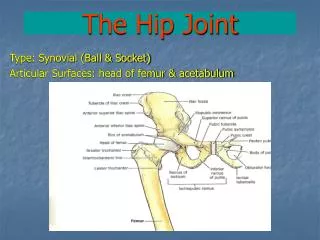
PATHOLOGY/ PATHOGENESIS: HIP JOINT • M.TB entry – inhalation, ingestion, skin innoculation • Primary complex, secondary spread and tertiary lesion • Always starts in bone, rarely synovium –granulomatous reaction • The anatomical sites of the lesions: • 1.The superior rim of the acetabulam • 2. Epiphysis • 3. Babcock's triangle • 4. Greater trochanter. • 5. Rarely, purely synovial in location. • In hip joint head and neck are intracapsular so a bony lesion invades the joint early
PATHOGENESIS cont. • If synovium is involved – marked effusion • Articular cartilage slowly destroyed • At synovial reflections there’s active bone erosion – increased vascularity • Secondary infection by pyogenic orgs common • If articular cartilage severely destroyed healing is by fibrous ankylosis • Within fibrocaseous mass mycobacteria may remain with potential of flare many years later
CLINICAL FEATURES • h/o previous TB infection or contact • Insidious onset, chronic course • Most pts are children • Prior constitutional symptoms • First symptom stiffness of hip with a limp • Pain may be absent in early stages • Pain worse at night – “night cries”
EXAMINATION • Look • Gait - stiff hip gait, antalgic, trendelenburg • Muscle wasting • Swelling due to cold abscess, Discharging sinuses • Flexion deformity, Limb length • Feel • Skin temperaturess, any swelling • Tenderness • Assess any pelvic tilt • Move • All mvts usually restricted due to pain and muscle spasm • Special tests • Thomas test • Bryant’s triangle/ Nelaton’s line • Galleazi’s test • Gauvain’s sign
The tuberculosis of hip mainly progresses through three stages .a- stage of synovitis ( FABER - AL )b- stage of arthritis ( FADIR - AS )c- stage of erosion ( FADIR - TS
Nelaton's line Bryant's triangle
INVESTIGATION • Haemogram –relative lymphocytosis • ESR • Mantoux test • Synovial fluid aspiration • AAFB positive in 10-20% of cases • Cultures positive in 50% of cases • Aspiration of cold abscess for microbiology • Synovial Biopsy • More reliable • Cultures positive in 80% of pts • Histology • Granulomatous inflammation/ caseous necrosis • Melon seed bodies
RADIOLOGY • Earliest sign • A general haziness of the bones • Normal joint space • An area of rarefaction in the babcock’s triangle • Increased joint space • Later • Lytic lesions with no or minimal reactive sclerosis • Travelling or wandering acetabulum • Posterior dislocation of the hip • Motor and pestle appearance • Protrusioacetabulare • Fibrous ankylosis
Note • A triad of radiologic abnormalities (Phemister triad); • periarticular osteoporosis • peripherally located osseous erosion • gradual diminution of joint space suggests the dx of TB • Occasionally, wedge-shaped areas of necrosis (kissing sequestra) in joint margin. These marginal erosions may simulate RA
TREATMENT • Rest • Chemotherapy • Arthroplasty • Arthrodesis • Osteotomy
TREATMENT: REST • Thomas urged that TB should be treated by rest – which had to be ‘prolonged, uninterrupted, rigid and enforced’. Hugh Owen Thomas
Treatment; Rest • Traction • Provides rest of the joint • Relieves muscle spasm • Prevents and corrects deformity • Maintains joint space • Minimises chance of developing wandering acetabulum
Arthroplasty • THR • Issues • Reactivation of disease • Duration of dz free interval before arthroplasty • Anti-TB use peri-arthroplasty • Excision arthroplasty
Arthrodesis • Possible option in a young pt with deformed hip • Brittain’s arthrodesis of the hip
References • Campbells operative orthopaedics • Appleys system of orthopaedics and fractures • 2009 TB guidelines by ministry of health • ROBERT JOHNSON, K. L. BARNES, R. OWEN Froni REACTIVATION OF TUBERCULOSIS AFTER TOTAL HIP REPLACEMENT • Qiaojie Wang, MD; Hao Shen, MD; Yao Jiang, MD; Qi Wang, MD; Yunsu Chen, MD; Junjie Shao, MD; Xianlong Zhang, MD CEMENTLESS tha IN ADVANCED TUBRCULOSISI OF THE HIP