Download
1 / 38
400 likes | 661 Views
Thyroid, Parathyroid, and Adrenal . Thyroid. arises as an outpouching of the primitive foregut around the third week of gestation originates at the base of the tongue at the foramen cecum

E N D
Thyroid • arises as an outpouching of the primitive foregut around the third week of gestation • originates at the base of the tongue at the foramen cecum • During its descent, the anlage remains connected to the foramen cecum via an epithelial-lined tube known as the thyroglossal duct • paired lateral anlages originate from the fourth branchial pouch and fuse with the median anlage at approximately the fifth week of gestation. The lateral anlages are neuroectodermal in origin (ultimobranchial bodies) and provide the calcitonin producing parafollicular or C cells
Developmental Abnormalities • Thyroglossal Duct Cyst and Sinus • may occur anywhere along the migratory path of the thyroid • 80% are found in juxtaposition to the hyoid bone • usually asymptomatic but occasionally become infected by oral bacteria, prompting the patient to seek medical advice • midline neck mass that moves upward with protrusion of the tongue. • Sistrunk = which consists of en bloc cystectomy and excision of the central hyoid bone • Lingual Thyroid • failure of the median thyroid anlage to descend normally • Intervention necessary for obstructive symptoms such as choking, dysphagia, airway obstruction, or hemorrhage • Surgical excision rarely needed should be preceded by an evaluation of normal thyroid tissue in the neck to avoid inadvertently rendering the patient hypothyroid.
Evaluation • TSH is only necessary test • Thyrotropin-Releasing Hormone to evaluate pituitary function • Thyroid antibodies • Radionuclide Imaging • Ultrasound • CT or MRI scans
Benign Thyroid Disorders • Diffuse Toxic Goiter (Graves' Disease) • Antibodies against TSH receptor • MCC of hyperthyroidism in US • Strong familial predisposition • Conditions such as the postpartum state, iodine excess, lithium therapy, and bacterial and viral infections have been suggested as possible triggers • Sx: palpitations, nervousness, fatigue, emotional lability, hyperkinesis, GI complaints • Suppressed TSH with elevated T3, T4 • Tx: antithryroid drugs, radioactive idoine, ablation, surgery when others fail or contraindicated or suspicious nodule • Toxic Multinodular Goiter • often have a prior history of a nontoxic multinodular goiter • thyroid nodules become autonomous to cause hyperthyroidism. • See suppressed TSH level and elevated free T4 or T3 levels • RAI uptake also is increased, showing multiple nodules with increased uptake and suppression of the remaining gland. • Subtotal thyroidectomy is the gold standard
Thyroid Storm • Hyperthyroidism accompanied by fever, central nervous system agitation or depression, cardiovascular dysfunction • Beta blockers • reduce peripheral T4 to T3 conversion • decrease the hyperthyroid symptoms. • Oxygen supplementation and hemodynamic support • Lugol's iodine • decrease iodine uptake and thyroid hormone secretion. • PTU blocks the formation of new thyroid hormone
Acute Thyroiditis • = SuppurativeThyroiditis • Infectious agents can seed it from the • hematogenous or lymphatic route • via direct spread from persistent pyriform sinus fistulae or thyroglossal duct cysts • penetrating trauma to the thyroid gland • due to immunosuppression. • Streptococcus and anaerobes account for about 70% of cases; • Acute suppurativethyroiditis is more common in children • preceded by an upper respiratory tract infection or otitis media • Treatment consists of IV antibiotics and drainage of abscesses.
SubacuteThyroiditis • Painful or painless forms • Painful thyroiditis thought to be viral in origin • Thyroiditis most commonly occurs in 30- to 40-year-old women • History of a preceding upper respiratory tract infection often can be elicited. • In the early stages of the disease, TSH is decreased, and T4 , and T3 levels are elevated due to the release of preformed thyroid hormone from destroyed follicles. • Painless thyroiditis is considered to be autoimmune in origin
Chronic Thyroiditis • The most common inflammatory disorder of the thyroid and the leading cause of hypothyroidism. • Hashimoto's thyroiditis = autoimmune process that • activation of CD4+ T (helper) lymphocytes with specificity for thyroid antigens • T cells can recruit cytotoxic CD8+ T cells to the thyroid • autoantibodies, which lead to complement fixation and killing by natural killer cells • More common in women between the ages of 30 and 50 years old. • An elevated TSH and the presence of thyroid autoantibodies • FNAB is indicated in patients who present with a solitary suspicious nodule or a rapidly enlarging goiter. • Treatment • Thyroid hormone replacement therapy is indicated in overtly hypothyroid patients, with a goal of maintaining normal TSH levels.
Riedel’s Thyroiditis • replacement of all or part of the thyroid parenchyma by fibrous tissue • etiology of this disorder is controversial • predominantly in women between the ages of 30 to 60 years old • presents as a painless, hard anterior neck mass, which progresses over weeks to years to produce symptoms of compression, including dysphagia, dyspnea, choking, and hoarseness. • Patients may present with symptoms of hypothyroidism and hypoparathyroidism as the gland is replaced by fibrous tissue • Surgery is mainstay of treatment
Solitary Nodule • 4% of individuals in the United States • Assess symptoms • Determine family history • risk factor for the development of both medullary and nonmedullary thyroid cancer • Do PE • best palpated from behind the patient and with the neck in mild extension. • Then proceed to further tests…
Papillary Cancer • 80% of all thyroid malignancies • predominant thyroid cancer in children and individuals exposed to external radiation. • Lymph node metastases are common, • Orphan Annie nuclei • Psammoma bodies • Excellent prognosis with a >95% 10-year survival rate. • AGES scoring system • Age, • histologicGrade, • Extrathyroidal invasion • metastases and tumor Size • Low versus High risk patients • If any high-risk factors total or near-total thyroidectomy. • If minimal papillary thyroid carcinoma in removed for other reasons, unilateral thyroid lobectomy and isthmusectomy is usually enough .
Follicular Cancer • 10% of thyroid cancers • Limitations inherent to FNAB diagnosis • Usually are solitary lesions, and the majority are surrounded by a capsule. • Treatment • Thyroid lobectomy because at least 80% of these patients will have benign adenomas. • Intraoperative frozen-section examination usually is not helpful • Total thyroidectomy should be performed when thyroid cancer is diagnosed
Postop Management • Stop T4 therapy for 4-6 weeks • Radioactive Iodine Scan look for hot spot • Adjuvant treatment with radioactive iodine • Then resume thyroid replacement therapy, will help supress • Can follow thyroglobulin measurement as marker • Screening ultrasound periodically to evaluate central and lateral neck compartments
Medullary Carcinoma • 5% of thyroid malignancies and arises from the parafollicular or C cells of the thyroid, • 25% occur within the spectrum of several inherited syndromes such as familial MTC, MEN2A, and MEN2B. • germline mutations in the RET proto-oncogene. • Present with neck mass, lymphadenopathy in 15-20% • Hematogenous spread • Unilateral if sporadic, multifocal if familial • Amyloid on slides • Screen for MEN! • Treat pheochromocytoma first • Total thyroidectomy with bilateral central neck dissection • Followup measure calcitonin and cEA • 10 yr survival 80% • Perform prophylactic thyroidectomy for MEN2 with RET
Anaplastic Thyroid Cancer • 1 % of thyroid malignancies in US • Women more common • Classic: long standing neck mass that rapidly enlarges and becomes painful • Sx: dysphonia, dysphagia, and dyspnea • May be fixed to surrounding structures or may be ulcerated with areas of necrosis • Confirmed by FNA • Isthmusectomy with or without a tracheostomy may be needed to alleviate tracheal obstruction. • Treatment and Prognosis • most aggressive thyroid malignancy • few patients surviving 6 months • Combined radiation and chemotherapy in patients with resectable disease has been associated with prolonged
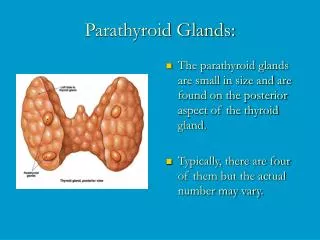
Parathyroid • Superior glands from the fourth branchial pouch (also thyroid gland) • Inferior glands form third branchial pouch (also thymus) • The position of normal superior parathyroid glands is more consistent • with 80% of these glands being found near the posterior aspect of the upper and middle thyroid lobes, • Approximately 15% of inferior glands are found in the thymus. • Undescended inferior glands may be found • near the skull base, • angle of the mandible, • frequency of intrathyroidal glands is about 2%.
Parathyroid Physiology • Rely on a G-protein coupled membrane receptor to regulate PTH secretion by sensing extracellular calcium levels • PTH secretion also stimulated by low levels of 1,25-dihydroxy vitamin D, catecholamines, and hypomagnesemia. • Secreted PTH has a half-life of 2 to 4 minutes. • PTH functions to regulate calcium levels via its actions on three target organs: • Bone • Kidney • Gut • Calcitonin produced by thyroid C cells antihypercalcemic hormone • inhibits osteoclast-mediated bone resorption. • Vitamin D refers to vitamin D2 and vitamin D3 , • both produced by photolysis of naturally occurring sterol precursors • Vitamin D is metabolized in the liver to its primary circulating form, 25-hydroxyvitamin D. • Further hydroxylation 1,25-dihydroxy vitamin D most metabolically active • Vitamin D stimulates the absorption of calcium and phosphate from the gut and the resorption of calcium from the bone.
Primary Hyperparathyroidism • Most cases of PHPT are sporadic. • Occurs within the spectrum of a number o inherited disorders such as MEN1, MEN2A, isolated familial HPT • Hyperplasia, Adenoma, Carcinoma • PHPT is the earliest and most common manifestation of MEN1 • 80 to 100% of patients by age 40 years old • Sx: kidney stones, painful bones, abdominal groans, psychic moans, and fatigue overtones • More likely to be asymptomatic and picked up on blood tests • Measure PTH to decide between the 2 causes of hypercalcemia • Surgery for complications, classic symptoms, age < 50 • Total versus focused • Localization studies: ultrasound, Sestamibi scan
Parathyroid Carcinoma • 1% of PHPT cases. • Suspect by preoperatively by the presence of severe symptoms • serum calcium levels >14 mg/dL • significantly elevated PTH levels (5 x normal) • palpable parathyroid gland • Local invasion is most common • Treatment • bilateral neck exploration, with en bloc excision of the tumor and the ipsilateral thyroid lobe. • Modified radical neck dissection if lymphadeonopathy
Hypercalcemic Crisis • Uncontrolled PTH secretion, • worsened by polyuria, dehydration, and reduced kidney function • Treatment consists of therapies to lower serum calcium levels followed by surgery • The mainstay of therapy involves rehydration • diuresis with furosemide • Further bisphosphonates, etc
Parathyroid Surgery • Asymptomatic Patient • Serum Ca > 1 mg/dl Above upper limits of normal • Life threatening hypercalcemic episode • Reduced creatinine clearance • Renal stones on xray • Markedley elevated 24 hour urine Ca • Substantially decreased bone mineral density
Secondary Hyperparathyroidism • commonly occurs in patients with chronic renal failure but also may occur in those with hypocalcemia secondary to inadequate calcium or vitamin D intake, or malabsorption. • The pathophysiology related to hyperphosphatemia, deficiency of 1,25-dihydroxy vitamin D due to loss of renal tissue, low calcium intake, decreased calcium absorption, and abnormal parathyroid cell response • generally hypocalcemic or normocalcemic. • treated medically with a low-phosphate diet, phosphate binders, adequate intake of calcium and 1,25-dihydroxy vitamin D and a high calcium, low-aluminum dialysis bath. • Surgery if: • bone pain, pruritus, calcium >11 mg/dL with markedly elevated PTH, calciphylaxis • A bilateral neck exploration is indicated • Consider subtotal resection with autotransplant
Tertiary Hyperparathyroidism • some patients develop autonomous parathyroid gland function and tertiary HPT after renal transplant • pathologic fractures, bone pain, renal stones, mental status changes. • Surgery if persists 1 year after transplant
Parathyroid Complications • Hypocalcemia • Vocal cord paralysis • Hypoparathyroidism • Permanent if > 6 mths
Adrenal • Outer cortex and an inner medulla • The cortex originates from mesodermal tissue near the gonads • Ectopic adrenocortical tissue may be found in the ovaries, spermatic cord, and testes. • Adrenal medulla is ectodermal in origin and arises from the neural crest. • Most extra-adrenal neural tissue regresses but may persist at several sites. • The largest of these ia left of the aortic bifurcation near the inferior mesenteric artery origin and is designated as the organ of Zuckerkandl.
Hyperaldosteronism • Secondary causes from stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow states such as congestive heart failure and cirrhosis. • Primary hyperaldosteronism results from autonomous aldosterone secretion which, I • leads to suppression of renin secretion. • 1% of hypertension cases. • Hypokalemia • Causes: • Adenoma 70% • Hyperplasia 30% • Carcinoma rare • Sx: hypertension difficult to control despite multiple-drug therapy, muscle weakness, polydipsia, polyuria, nocturia, headaches, and fatigue. • Labs: K+. Measure renin-aldosterone • CT scan can localize with sensitivity of 90% • Selective venous sampling • Txs: • spironolactone (aldosterone antagonist) • amiloride (a potassium-sparing diuretic that blocks sodium channels in the distal nephron • nifedipine • Captopril • Unilateral tumors producing aldosterone are best managed by adrenalectomy
Cushing Syndrome • Hypercortisolism • Most common cause iatrogenic • 70% are pituitary tumor, 20% adrenal tumor, 10% ectopic ACTH producing tumor • Sx: wt gain, buffalo hump, central obesity, striae, acne, hypertension, neurologic or pyschiatric disorders • elevated glucocorticoid levels that are not suppressible by exogenous hormone administration and loss of diurnal variation • overnight low-dose dexamethasone suppression test. In this test • Cushing's syndrome patients do not suppress • Measure ACTH to determine if ACTH dependent; • If ACTH dependent do high dose dexamethoasone test; if no supression then likely ectopic • Laparoscopic adrenalectomy is the treatment of choice for patients with adrenal adenomas. • Open adrenalectomy for large tumors (≥6 cm) or those suspected to be adrenocortical cancers • Cushing disease treatment is transsphenoidal excision • May need mineralocorticoid and glucocorticoid replacement therapy
Congenital Adrenal Hyperplasia • Deficiencies or complete absence of enzymes involved in adrenal steroidogenesis. • 21-Hydroxylase deficiency is the most common enzymatic defect (>90% of cases) • overproduction of adrenal androgens and corticosteroid precursors such as 17-hydroxyprogesterone and androstenedione. • converted to testosterone in the peripheral tissues, thereby leading to virilization. • Complete deficiency of 21-hydroxylase presents at birth with: virilization, diarrhea, hypovolemia, hyponatremia, hyperkalemia, and hyperpigmentation. • Dx: karyotype and measurement of plasma and urinary steroids • Tx: traditionally have been managed medically with cortisol and mineralocorticoid replacement to suppress the hypothalamic-pituitary-adrenal axis. • teroids required often are supraphysiologic lead to iatrogenic hypercortisolism lap adrenalectomy gaining momentum
Pheochromocytoma • Disorders of the Adrenal Medulla; paraganglioma if extra adrenal • 10 percent tumor because • 10% are bilateral, 10% are malignant, 10% occur in pediatric patients, 10% are extra-adrenal, and 10% are familial. • Pheochromocytomas occur in families with MEN2A and MEN2B • Sx: Headache, palpitations, and diaphoresis • Dx: 24 hr urine for catecholamines and plasma metanephrines • CT to localize tumor • Need alpha blocker first, titrate to orthostatic hypotension • Adrenalectomy is treatment of choice • 12-29% are malignant, and these tumors are associated with decreased
Adrenal Insufficiency • May be primary, resulting from adrenal disease, or secondary, due to a deficiency of ACTH • The most commonly encountered causes of primary adrenal insufficiency are autoimmune disease, infections, and metastatic deposits. • fulminant meningococcal septicemia (Waterhouse-Friderichsen syndrome). • Bilateral adrenal hemorrhage also can occur secondary to trauma, severe stress, infection, and coagulopathies and, if unrecognized, is lethal. • Suspect in stressed patients with any of the relevant risk factors • laboratory findings: hyponatremia, hyperkalemia, fasting or reactive hypoglycemia • ACTH stim test • Peak cortisol levels <20 g/dL suggest adrenal insufficiency • Replace glucocorticoids and mineralocorticoids
Adrenal Complications • Postoperative hemodynamic instability • pheochromocytomas • Nelson's syndrome from progressive growth • increased ACTH levels • hyperpigmentation, • extraocular muscle palsies.
You are seeing a postop total parathyroidectomy patient who complains of SOB. What do you do?
A patient is diagnosed with medullary thyroid cancer, what should you do prior to surgery?
What are the complications of thyroidectomy or parathyroidectomy?