Download
1 / 64
640 likes | 929 Views
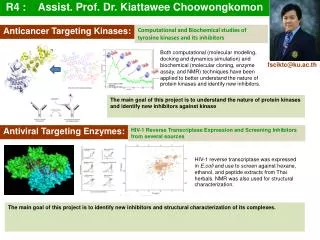
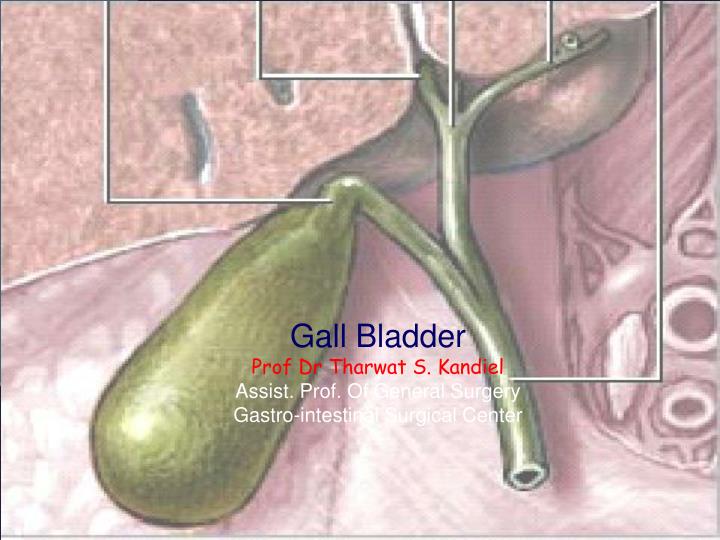
Gall Bladder Prof Dr Tharwat S. Kandiel Assist. Prof. Of General Surgery Gastro-intestinal Surgical Center. Anatomy. The gallbladder (or cholecyst, sometimes gall bladder) is a pear-shaped organ that stores about 50 mL of bile (or "gall") until the body needs it for digestion. Anatomy.

E N D
Gall Bladder Prof Dr Tharwat S. Kandiel Assist. Prof. Of General Surgery Gastro-intestinal Surgical Center
Anatomy • The gallbladder (or cholecyst, sometimes gall bladder) is a pear-shaped organ that stores about 50 mL of bile (or "gall") until the body needs it for digestion.
Anatomy The gallbladder is about 7-10 cm long in humans and appears dark green because of its contents (bile), rather than its tissue. It is connected to the liver and the duodenum by the biliary tract. • The cystic duct leads from the gallbladder and joins with the common hepatic duct to form the common bile duct. • The common bile duct then joins with the pancreatic duct, and enters the duodenum through the hepatopancreatic ampulla at the major duodenal papilla.
Histology The layers of the gallbladder are as follows: • The gallbladder has a simple columnar epithelial lining characterized by recesses called Aschoff's recesses (lacunae of Luschka) , which are pouches inside the lining. • Under the epithelium there is a layer of connective tissue. • Beneath the connective tissue is a wall of smooth muscle that contracts in response to cholecystokinin, a peptide hormone secreted by the duodenum. • There is essentially no submucosa.
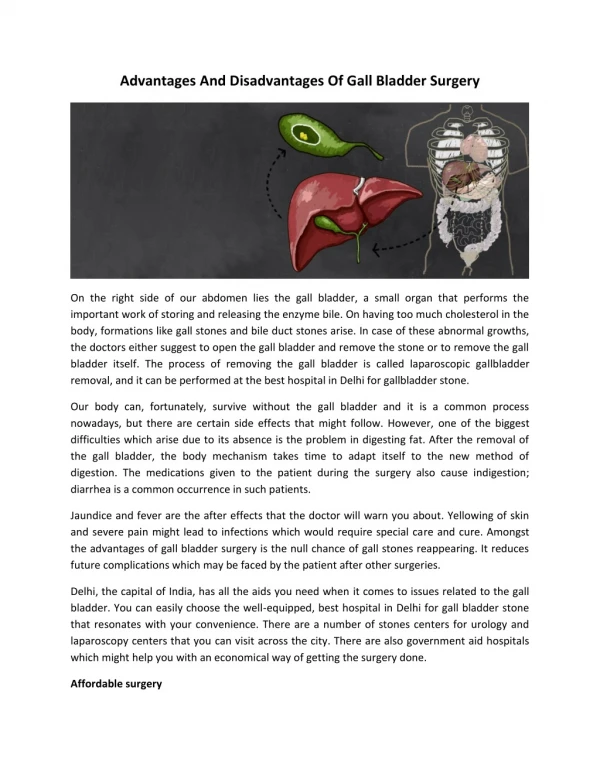
Function • The gallbladder stores about 50 mL of bile , which is released when food containing fat enters the digestive tract, stimulating the secretion of cholecystokinin (CCK). The bile, produced in the liver, emulsifies fats and neutralizes acids in partly digested food. • After being stored in the gallbladder, the bile becomes more concentrated than when it left the liver, increasing its potency and intensifying its effect on fats. Most digestion occurs in the duodenum.
Anomalies • The gallbladder may be absent = 0.075% • The gallbladder and cystic duct may be absence. • the gallbladder is irregular in form or constricted across its middle; more rarely, it is partially divided in a longitudinal direction. • two distinct gallbladders, each having a cystic duct that joined the hepatic duct. (0.026%), The cystic duct may itself be doubled • The gallbladder has been found on the left side (to the left of the ligamentum teres) in subjects in whom there was no general tranposition of the thoracic and abdominal viscera.
The gallbladder may be intrahepatic or beneath the left lobe. Ectopic sites include retrohepatic positions, or in the anterior abdominal wall or falciform ligament, they may be suprahepatic or transversely position, floating, or retroperitoneal. They may be in the midline anterior epigastric above the left lobe or suprahepatic above the right hepatic lobe.
Choledochal cyst • Choledochal cysts are congenital anomalies of the bile ducts. They consist of cystic dilatations of the extrahepatic biliary tree, intrahepatic biliary radicles, or both. • Douglas is credited with the first clinical report in a 17-year-old girl who presented with intermittent abdominal pain, jaundice, fever, and a palpable abdominal mass. • Pathophysiology: The pathogenesis of choledochal cysts is most likely multifactorial. • A congenital etiology, • A congenital predisposition to acquiring the disease under the right conditions.
The vast majority of patients with choledochal cysts have an anomalous junction of the common bile duct with the pancreatic duct (anomalous pancreatobiliary junction [APBJ]). An APBJ is characterized when the pancreatic duct enters the common bile duct 1 cm or more proximal to where the common bile duct reaches the ampulla of Vater. • APBJs in more than 90% of patients with choledochal cysts.
The APBJ allows pancreatic secretions and enzymes to reflux into the common bile duct. In the relatively alkaline conditions found in the common bile duct, pancreatic pro-enzymes can become activated. This results in inflammation and weakening of the bile duct wall. Severe damage may result in complete denuding of the common bile duct mucosa.
From a congenital standpoint, defects in epithelialization and recanalization of the developing bile ducts during organogenesis and congenital weakness of the duct wall have also been implicated. The result is formation of a choledochal cyst.
Anatomy of Choledochal cyst based on the Todani classification published in 1977. • Type I choledochal cysts • most common ; 80-90% of the lesions. • Type I cysts are dilatations of the entire common hepatic and common bile ducts or segments of each. • They can be saccular or fusiform in configuration. • Type II choledochal cysts • isolated protrusions or diverticula that project from the common bile duct wall. They may be sessile or may be connected to the common bile duct by a narrow stalk.
Type III choledochal cysts are found in the intraduodenal portion of the common bile duct. Another term used for these cysts is choledochocele.
Type IVA cysts are characterized by multiple dilatations of the intrahepatic and extrahepatic biliary tree. Most frequently, a large solitary cyst of the extrahepatic duct is accompanied by multiple cysts of the intrahepatic ducts. Type IVB choledochal cysts consist of multiple dilatations that involve only the extrahepatic bile duct. • Type V choledochal cysts are defined by dilatation of the intrahepatic biliary radicles. Often, numerous cysts are present with interposed strictures that predispose the patient to intrahepatic stone formation, obstruction, and cholangitis. The cysts are typically found in both hepatic lobes. Occasionally, unilobar disease is found and most frequently involves the left lobe.
The patient may present at any age with • Obstructive jaundice • Cholangitis and • Abd signs, with RUQ swelling in some cases • It is a premalignant condition • Diagnosis by US and MRI • Radical excision of the cyst is the treatment of choice with Roux – en –Y reconstruction
Gall stones • Gall stones are the most common abdominal reason for admission to hospital in developed countries and account for an important part of healthcare expenditure. Around 5.5 million people have gall stones in the United Kingdom, and over 50 000 cholecystectomies are performed each year. • Normal bile consists of 70% bile salts (mainly cholic and chenodeoxycholic acids), 22% phospholipids (lecithin), 4% cholesterol, 3% proteins, and 0.3% bilirubin. • There are two major types of gallstones, which seem to form due to distinctly different pathogenetic mechanisms.
Cholesterol Stones • About 90% of gallstones are of this type. These stones can be either; • almost pure cholesterol {Cholesterol stones} • or mixtures of cholesterol and other substances{ cholesterol predominant (mixed) stones}.
The key event leading to formation and progression of cholesterol stones is precipitation of cholesterol in bile. • Unesterified cholesterol is virtually insoluble in aqueous solutions and is kept in solution in bile largely by virtue of the detergent-like effect of bile salts.
Imbalance lead to stone formation • Hyper-secretion of cholesterol into bile due to • obesity, • acute high calorie intake, • chronic polyunsaturated fat diet, contraceptive steroids or pregnancy, • diabetes mellitus and • certain forms of familial hypercholesterolemia.
Hypo-secretion of bile salts due to • impaired bile salt synthesis and • abnormal intestinal loss of bile salts (e.g. recirculation failure due to ileal disease). • Impaired gallbladder function with incomplete emptying or stasis. • seen in late pregnancy • with oral contraceptive use, • in patients on total parenteral nutrition and • due to unknown causes, perhaps associated with neuro-endocrine dysfunction.
There are clearly important genetic determinants for cholesterol stone formation. For example, the prevelance of the disease in descendents of Chilean, Indians and in American Indians is extraordinarily high and not accounted for by environment. • There is also an important sex bias in development of stones - the prevelance in adult females is two to three times that seen in males
Pigment Stones • Roughly 10% of gallstones are pigment stones composed of large quantities of bile pigments, along with lesser amounts of cholesterol and calcium salts. • Black pigment stones • consist of 70% calcium bilirubinate and are more common in patients with haemolytic diseases (sickle cell anaemia, hereditary spherocytosis, thalassaemia) and cirrhosis.
Brown pigment stones (accounting for <5% of stones) • They form as a result of stasis and infection within the biliary system, usually in the presence of Escherichia coli and Klebsiella spp, which produce β glucuronidase that converts soluble conjugated bilirubin back to the insoluble unconjugated state leading to the formation of soft, earthy, brown stones. • Ascaris lumbricoides and Opisthorchis senensis have both been implicated in the formation of these stones, which are common in South East Asia.
In the GB: Silent stones Chronic cholecystitis Acute cholecystitis Gangrene Perforation Empeyma Mucocele carcinoma In the bile ducts: Obstructive jaundice Cholangitis Acute pancreatitis In the intestine: Acute intestinal obstruction (Gall stone ileus) Effects and complications of Gall Stones
Cholecystitis Definition • Cholecystitis refers to a painful inflammation of the gallbladder's wall. The disorder can occur a single time (acute), or can recur multiple times (chronic). • Cholecystitis is defined as inflammation of the gallbladder that occurs most commonly because of an obstruction of the cystic duct from cholelithiasis. Ninety percent of cases involve stones in the cystic duct (ie, calculous cholecystitis), with the other 10% representing acalculous cholecystitis. Although bile cultures are positive for bacteria in 50-75% of cases, bacterial proliferation may be a result of cholecystitis and not the precipitating factor.
Causes • Risk factors for calculous cholecystitis mirror those for cholelithiasis and include the following: • Female sex • Certain ethnic groups (Race) • Obesity or rapid weight loss • Drugs (especially hormonal therapy in women) • Pregnancy • Increasing age
Acalculous cholecystitis is related to conditions associated with biliary stasis, to include the following: • Critical illness • Major surgery or severe trauma/burns • Sepsis • Long-term TPN • Prolonged fasting
Other causes of acalculous cholecystitis include the following: • Cardiac events, including myocardial infarction • Sickle cell disease • Salmonella infections • Diabetes mellitus • Patients with AIDS with cytomegalovirus, cryptosporidiosis, or microsporidiosis • Idiopathic cases exist.
History • Typical gallbladder colic is 1-5 hours of constant pain, most commonly in the epigastrium or right upper quadrant. Pain may radiate to the right scapular region or back. Peritoneal irritation by direct contact with the gallbladder localizes the pain to the right upper quadrant. Pain is severe, dull or boring, and constant (not colicky). Patients tend to move around to seek relief from the pain. Onset of pain develops hours after a meal, occurs frequently at night, and awakens the patient from sleep. • Associated symptoms include nausea, vomiting, pleuritic pain, and fever.
Indigestion, belching, bloating, and fatty food intolerance are thought to be typical symptoms of gallstones; however, these symptoms are just as common in people without gallstones and frequently are not cured by cholecystectomy.
Most gallstones (60-80%) are asymptomatic at a given time. Smaller stones are more likely to be symptomatic than larger ones. Almost all patients develop symptoms prior to complications. • Symptoms of cholecystitis are steady pain in the right hypochondrium or epigastrium, nausea, vomiting, and fever. Acute attack often is precipitated by a large or fatty meal.
Physical • Vital signs parallel the degree of illness. Patients with cholangitis are more likely to have fever, tachycardia, and/or hypotension. Patients with gallbladder colic have relatively normal vital signs. • Patients with cholecystitis are usually more ill appearing than simple biliary colic patients, and they usually lie still on the examination table since any movement may aggravate any peritoneal signs.
Abdominal examination; • Epigastric or RUQ tenderness and abdominal guarding. • The Murphy sign (an inspiratory pause on palpation of the right upper quadrant) can be found on abdominal examination. • Positive Murphy sign was extremely sensitive (97%) and predictive (PPV, 93%) for cholecystitis. However, in elderly patients, this sensitivity may be decreased.
peritoneal signs should be taken seriously. Most uncomplicated cholecystitis does not have peritoneal signs; thus, search for complications (eg, perforation, gangrene) or other sources of pain. • Gallbladder gangrene can be a complication in up to 20% of cases of cholecystitis and is usually in diabetics, elderly, or immunocompromised persons. • A palpable fullness in the RUQ may be appreciated in 20% of cases.
As in all patients with abdominal pain, perform a complete physical examination, including rectal and pelvic examinations in women. • In elderly patients and those with diabetes, occult cholecystitis or cholangitis may be the source of fever, sepsis, or mental status changes. • Jaundice is unusual in the early stages of acute cholecystitis and may be found in fewer than 20% of patients. • A very high bilirubin =think for common bile duct and pancreatic region disease.
Abdominal Aortic Aneurysm Acute Mesenteric Ischemia Amebic Hepatic Abscesses Appendicitis Biliary Colic Biliary Disease Cholangiocarcinoma Cholangitis Choledocholithiasis Cholelithiasis Gallbladder Cancer Gallbladder Mucocele Gallbladder Tumors Gastric Ulcers Gastritis, Acute Gastroesophageal Reflux Disease Hepatitis, Viral Myocardial Infarction Nephrolithiasis Pancreatitis, Acute Peptic Ulcer Disease Pneumonia, Bacterial Pregnancy and Urolithiasis Pyelonephritis, Acute Renal Disease and Pregnancy Renal Vein Thrombosis DD
Lab Studies • Labs with cholelithiasis and gallbladder colic should be completely normal. • Because biliary obstruction is limited to the gallbladder in uncomplicated cholecystitis, elevation in the serum total bilirubin and alkaline phosphatase concentrations may not be present. • An elevated WBC is expected but not reliable. Only 61% of patients with cholecystitis had a WBC greater than 11,000. A WBC greater than 15,000 may indicate perforation or gangrene.
Mild elevation of amylase up to 3 times normal may be found in cholecystitis, especially when gangrene is present. • Prothrombin time (PT) and activated partial thromboplastin time (aPTT) are not expected to be elevated unless sepsis or underlying cirrhosis is present. Coagulation profiles are helpful if the patient needs operative intervention. • For febrile patients, send 2 sets of blood cultures to attempt to isolate the organism. • Although expected to be normal, urinalysis is essential in the workup of patients with abdominal pain to exclude pyelonephritis and renal calculi. • Conduct a pregnancy test for women of childbearing age.
Imaging Studies • Ultrasound and nuclear medicine studies are the best imaging studies for the diagnosis of both cholecystitis and cholelithiasis. Plain radiography, CT scans, and endoscopic retrograde cholangiopancreatography (ERCP) are diagnostic adjuncts.
Abd. radiographs (Plain X-Ray) • Adominal radiographs have low sensitivity and specificity in evaluating biliary system pathology, but • They can be helpful in excluding other abdominal pathology such as renal colic, bowel obstruction, perforation. Between 10 and 30% of stones have a ring of calcium and, therefore, are radiopaque. A porcelain gallbladder also may be observed on plain films.
Emphysematous cholecystitis, cholangitis, cholecystic-enteric fistula, or postendoscopic manipulation may show air in the biliary tree. Air in the gallbladder wall indicates emphysematous cholecystitis due to gas-forming organisms such as clostridial species and Escherichia coli.
Computed tomography scan • CT scan is recommended only for the evaluation of abdominal pain if the diagnosis is uncertain. CT scan can demonstrate gallbladder wall edema, pericholecystic stranding and fluid, and high-attenuation bile. • Advantages: For complications of cholecystitis and cholangitis, gallbladder perforation, pericholecystic fluid, and intrahepatic ductal dilation, CT scan may be adequate. CT scan provides better information of the surrounding structures than sonogram and HIDA. CT scan is also noninvasive. • Disadvantages: CT scan misses 20% of gallstones because the stones may be of the same radiographic density as bile. CT scan is also more expensive and takes longer since the patient usually has to drink oral contrast. Also, given the radiation dose, it may not be ideal in the pregnant patient.
Ultrasound • An ultrasound is the most common test used for the diagnosis of biliary colic and acute cholecystitis. It is 90-95% sensitive for cholecystitis and 78-80% specific. For simple cholelithiasis, it is 98% sensitive and specific.
Findings include gallstones or sludge and one or more of the following conditions • Gallbladder wall thickening (>2-4 mm) - False-positive wall thickening found in hypoalbuminemia, ascites, congestive heart failure, and carcinoma • Gallbladder distention (diameter >4 cm, length >10 cm) • Pericholecystic fluid from perforation or exudate • Air in the gallbladder wall (indicating gangrenous cholecystitis) • Sonographic Murphy sign (86-92% sensitive, 35% specific), pain when the probe is pushed directly on the gallbladder (not related to breathing)
Some sonographers recommend the diagnosis of cholecystitis if both a sonographic Murphy sign and gallstones (without evidence of other pathology) are present. • Additional findings in the presence or absence of gallstones: Dilated common bile duct or dilated intrahepatic ducts of the biliary tree indicate common bile duct stones. In the absence of stones, a solitary stone may be lodged in the common bile duct, a location difficult to visualize sonographically.
Advantages of sonography include the following: • Images other structures (eg, aorta, pancreas, liver) • Identifies complications (eg, perforation, empyema, abscess) • Rapidly performed at the bedside • No radiation (important in pregnancy) • Disadvantages of sonography include the following: • Operator dependent and patient dependent • Inability to image the cystic duct • Decreased sensitivity for common bile duct stones
Biliary scintigraphy (HIDA, diisopropyl iminodiacetic acid [DISIDA]), nuclear medicine studies • Sonography or nuclear medicine testing is the test of choice for cholecystitis. HIDA scans have sensitivity (94%) and specificity (65-85%) for acute cholecystitis. They are sensitive (65%) and specific (6%) for chronic cholecystitis. Oral cholecystography is not practical for the ED. • HIDA and DISIDA scans are functional studies of the gallbladder. Technetium-labeled analogues of iminodiacetic acid (IDA) or diisopropyl IDA-DISIDA are administered intravenously (IV) and secreted by hepatocytes into bile, enabling visualization of the liver and biliary tree.