Download
1 / 34
340 likes | 361 Views
Learn about risk prediction tools in primary care, including QRISK for CVD, QDScore for diabetes, and QKidney for CKD, to enable informed decisions and better patient care. This initiative integrates scientific credibility, clinical relevance, and adaptability to NHS needs.

E N D
QScores: SupportingVascular Risk Assesessment Julia Hippisley-Cox 01 July 2010 London
Acknowledgements Practices contributing data to QResearch database Many GPs & nurses for suggestions, piloting EMIS - QResearch database & piloting Academic colleagues THIN (validation data) Oxford University – independent validation ClinRisk Ltd (software) NICE (stimulating debate!)
Outline • Overview risk prediction in primary care • Vascular Risk Engine • Cardiovascular disease - QRISK • Diabetes - QDScore • Chronic Kidney Disease - QKidney • Risks and benefits interventions - QIntervention
See www.qresearch.org for Information about QResearch database Academic papers Technical & statistical documents Open source software Patient information Clinician information Power points presentations
New research paradigm • Moving from ivory tower • I wonder whether ... • I have a hunch (“hypothesis”) to test • Moving into real world NHS • Who is most at risk of preventable disease? • Who is likely to benefit from interventions? • What is the balance of risks and benefits for my patient? • Enable informed consent and shared decisions
Change in research question • Leads to • Novel application of existing methods • Development of new methods • Better utilisation different data sources • Leads to • Lively academic debate! • Changes in policy and guidance • New utilities to implement research findings • (hopefully) better patient care
The Research Cycle‘clinically useful epidemiology - new knowledge & utilities to improve patient care’
Risk prediction tools needed • Population level • Risk stratification • Identification of rank ordered list of patients for recall or reassurance • Individual assessment • Baseline risk of disease/outcome • Risks and benefits of interventions • Needed to obtain informed consent from patients
Framingham 1970’s Our diverse UK population in 2010 Why develop new tools?
Why develop in primary care? Huge scope for risk prediction models in primary care High levels of computerisation Unselected, large representative cohorts Good quality databases Detailed event level data for outcomes &predictors Longitudinal data > 15 years Linked ONS mortality data Huge potential for decision support
Why integrated tool CVD, diabetes, CKD? • Many of the risk factors over overlap • Many of the interventions overlap • But different patients have different risk profiles • Smoking biggest impact on CVD risk • Obesity has biggest impact on diabetes risk • Blood pressure biggest impact on CKD risk • Help set individual priorities • Development of personalised plans and achievable target
Vascular Risk Engine: Requirements • Identify patients at high risk of vascular disease • CVD • Diabetes • Stage 3b,4, 5 Kidney Disease • Assessment of individual’s risk profile • Risks and benefits of interventions • Weight loss • Smoking cessation • BP control • Statins
Vascular Risk Engine: 10 Requirements Scientificallysound –peer reviewed, validated Appropriate for context & decade Accurate identify higher & lower risk patient Sociallyequitable Clinicallyrelevant – include relevant risk factors, obesity, family history, comorbidity
Vascular Risk Engine: 10 Requirements 6. Practical –used in busy clinics 7. Available - stand alone & integrated into systems 8. Consistent - “same patient same score anywhere” 9. Updatable - to reflect changes in populations & data & advances in methodology 10. Adaptable - as NHS requirements change • 10 Year risk • Life Time Risk • Measures of Relative Risk – Heart age etc
QRISK2 - www.qrisk.org Risk of CVD – 1-15 years & lifetime Extensively reviewed and externally validated Included in QOF, NICE, DH Vascular Guidance Widespread use across NHS Incorporated into nearly all GP systems, many pharmacies, some hospitals, NHS Choices, Occupational Health etc Available as Open Source and Closed Software
QRISK – Lifetime Risk NICE guidance based on absolute 10 year risk ie chance of having an event over next 10 years QRISK model is very flexible QRISK can calculate risk over any age or time period QRISK Lifetime Risk is an alternative to 10 year risk Example: If you are 35, your lifetime risk is the risk of developing CVD by age 99 assuming you live that long.
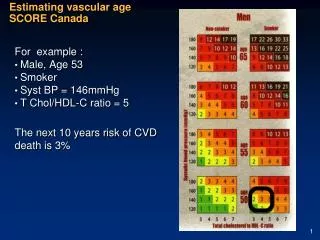
Life time risk - example 50 year old man Heavy smoker SBP=190 cholesterol ratio=7.8 10 year risk = 18% Lifetime risk= 48%
Growth in prevalent patients by RRT at the end of each year 1982-2007
Identifying people with or at risk of CKD Identify who needs intervention to minimise CV risk Identify progressive CKD and how to manage it Identify who needs referral for specialist kidney care
QKidney-why focus high risk CKD3b+? Kidney is twice as important as we have two (renal tsar!) Optimise early management Prevention of progression Prevention of complications Reduce late referral – cause of avoidable harm Optimise use of resources in our Health Services The right patient in the right place at the right time
So developed QKidneyScores • Set of algorithms • Identifies those at risk of developing CKD3b+ • Those at risk of deteriorating • So we can then • Identify high risk • Modify risk factors • Avoid nephrotoxic drugs • Monitor more closely • Hopefully prevent deteriorating • Improve outcomes
QDScore – risk of Type 2 diabetes Predicts risk of type 2 diabetes Published in BMJ (2009) Independent external validation by Oxford Uni Needed as epidemic of diabetes & obesity Evidence diabetes can be prevented Evidence that earlier diagnoses associated with better prognosis.
QRISK CVD • Cholesterol ratio • FHCHD • Atrial Fibrillation • SBP • Diabetes • Rheumatoid • Common risk factors • Age • Deprivation • Ethnicity • Smoking • Hypertension • Body Mass index • QKidney – stage 3b,4,5 • FH Kidney Disease • CCF • PVD • Rheumatoid • SLE • Kidney stones • NSAIDS • SBP • Diabetes • CVD • QDScore (Diabetes) • FH of Diabetes • Steroid tablets • CVD • Common interventions • Smoking cessation • Weight loss • BP control • Exercise • Lipid lowering • Etc
Primary prevention CVD:(slide from NICE website) • Offer information about: • absolute risk of CVD • absolute benefits/harms of an • intervention over a 10-year period • Information should: • present individualised risk/benefit • scenarios • present absolute risk of events • numerically • use appropriate diagrams and text
But the task in the consultation is to Undertake clinical assessment Work out individual’s risk of disease Calculate expected risks and benefits from interventions Explain risks and benefits to an individual in a way they can understand Draw some diagrams All within 10 minutes!
Risks and Benefits Statins • Two recent papers: • Unintended effects statins BMJ (2010) • Individualising Risks and Benefits of Statins Heart (2010) • Conclusions: • New tools to quantify likely benefit from statins • New tools to identify patients who might get rare adverse effects eg myopathy for closer monitoring
New approach, new models, new utilities • At population level • Risk stratification so identify and recall high risk patients CVD, diabetes, CKD3b+ • Must be fit for purpose - scientifically robust, practical and automated • At patient level • Calculation of risk and benefits for the individual • Help inform decision making • Better more individualised informed care
QScores: SupportingVascular Risk Assesessment Julia Hippisley-Cox 01 July 2010 London