Download
1 / 17
370 likes | 2.65k Views
Adenoviridae. Nonenveloped, hexagonal virions with icosahedral capsid ~80-100 nm in diameter Genome consists of a DS linear DNA Virions replicate in nucleus; release of progeny virions occur via cell lysis

E N D
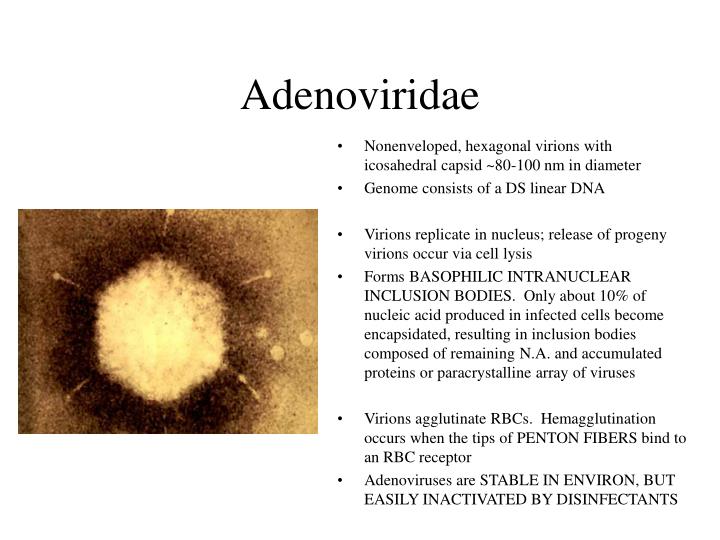
Adenoviridae • Nonenveloped, hexagonal virions with icosahedral capsid ~80-100 nm in diameter • Genome consists of a DS linear DNA • Virions replicate in nucleus; release of progeny virions occur via cell lysis • Forms BASOPHILIC INTRANUCLEAR INCLUSION BODIES. Only about 10% of nucleic acid produced in infected cells become encapsidated, resulting in inclusion bodies composed of remaining N.A. and accumulated proteins or paracrystalline array of viruses • Virions agglutinate RBCs. Hemagglutination occurs when the tips of PENTON FIBERS bind to an RBC receptor • Adenoviruses are STABLE IN ENVIRON, BUT EASILY INACTIVATED BY DISINFECTANTS
Adenoviridae • Virion shows penton fiber peplomeres from the vertices • Crystalline array of virions in host cell nucleus • Penton fiber knobs contain cell binding ligands that are responsible for viral attacdhment to host cell receptors, • Associated with hemagglutinating activity • Genera – • Mastadenovirus – Mammalina adenoviruses • Single penton fiber from vertex • Aviadenovirus – Avian adenoviruses • Each penton is bifurcated – giving the appearance of 2 fibers extending from each penton base
Adenoviridae - pathogenesis • All adenoviruses- NARROW HOST RANGE – HIGHLY HOST SPECIFIC • MOSTLY SUBLICINICAL INFECTIONS WITH OCCASIONAL URT INFECTIONS, GI TRACT DISEASES • Virus persists in the pharyngeal region, particularly associated with the lymphoid tissues oin respiratory infections nad in the GALT tissues – enteric infections • Several adenoviruses ARE PATHOGENIC in IMMUNODEFICIENT ANIMALS like Arabian foals with SEVERE COMBINED IMMUNNODEFICIENCY – SCID
Adenovirus – Infectious canine Hepatitis • Infectious Canine Hepatitis – ICH – Rubarth’s Disease (tonsilitis at left) • Rubarth’s Disease – Dr. Rubarth’s distinguished it from Canine Distemper virus using ferrets that are resistant to ICH, but not to Canine Distemper • ICH is worldwide in occurrence • Hosts – Family Canidae – domestic and wild, Ursidae – bears • Etiologic agent – canine adenovirus 1 – one serotype. • CAV-1 is antigenically related to but distinct from CAV-2
Adenovirus – Infectious Canine Hepatitis • Disinfecting agents – • STABLE VIRUS – lives for days at room temp. And months at less than 4 degrees C. • CAV-1 is susceptible to iodine, phenol, NaOH and bleach • Transmission – • Present in respiratory secretions, urine, feces, and saliva • Recovered dogs shed virus in urine for >6 months/ longest time 9 months • Ingestion of urine, feces or saliva of infected dogs is the main route of infection. However, virus may be acquired via CONJUNCTIVAL OR AEROSOL ROUTES
Adenovirus – Infectious Canine Hepatitis • Pathogenesis – • Occurs in the tonsillar crypts and Peyers patches – INITIAL SITE OF INFECTION • See left – tonsilitis of dog infected • There is viremia of 4-8 days duration and infection of MACS, ENDOTHELIAL CELLS AND PARENCHYMAL CELLS in many tissues, leading to HEMORRHAGES AND NECROSIS • LIVER, KIDNEYS, SPLEEN, LUNGS ARE MAIN TARGETS
Infectious Canine Hepatitis • Initial cell injury of liver, kidney are eye are associated with cytotoxic effects of virus • Sufficient neutralizing antibody response by day 7 PI >1:500 clears the virus from the blood and liver and restricts the extent of hepatic damage • Antibody titer < 1:4 • Widespread hepatic necrosis • Partial immunity >1:16 <1:500 – Dogs may develop chronic active hepatitis and hepatic fibrosis
Infectious Canine Hepatitis • We know the exact antibody titer to protect the animal 1/500 level in colostrum, vaccine response – should be protected • Virus spread flow chart explanation: START…. • Virus --- tonsils ---Cervical lymph nodes ---- thoracic duct ---- blood (viremia) • From the viremic phase four target sites: • 1. Eye --- uvea, anterior chamber corneal endothelium ---IMMUNE COMPLEX, severe uveitis, corneal edema –two outcomes : spontaneous resolution or glaucoma, keratoconus, hydrophthalmos, phthisis bulbi • 2.Liver ---kupffer cells, hepatocytes--- • Low titer ---centrolobular necrosis – acute death or acute hepatitis and begin to recover • High titer – chronic hepatitis --- chronic hepatic fibrosis – cirrhosis OR mild or inapparent disease • 3. Kidney – glomerular endothelium --- immune complex glomerulonephritis --- focal interstitial nephritis (viruria) --- can shed for 9 months • 4. Endothelium (brain, lungs, lymph nodes) excreted in feces, saliva --- organ failure- DIC and death OR virus cleared from tissues and recovery
Infectious Canine Hepatitis – Corneal Edema – Blue Eye • Adenovirus – result of corneal edema due to uveitis secondary to immune complex deposition • Occurs in about 20% of , severe natural infectious an less than 1% of dogs after SC-MLV CAV-1 vaccination • Homologous vaccine is always stronger than heterologous • Can treat with atropine and corticosteroids • Occurs during the recovery phase of the antibody-mediated disease – moderate response • On day 4, virus enters aqueous humor from blood and replicates in corneal endothelial cells • By day 7, severe anterior uveitis and corneal edema develop. • Circulating immune complexes deposited on the corneal endothelium – IMMUNE COMPLEX HYPERSENSITIVITY
Infectious Canine Hepatitis – Corneal Edema,Glomerulonephritis • Circulating immune complexes deposited on the corneal endothelium result in: • Classical Pathway Complement activation • Neutrophil chemotaxis • Frustrated phagocytosis • Corneal endothelial damage • Disruption of the corneal endothelium results in accumulation of edematous fluid in the corneal stroma • Usually self-limiting • From day 8-21 MACS remove immune complexes and corneal endothelium regenerates, re-establishing the hydrotatic gradient • Kidney – glomerulonephritis – Chronic kidney lesions result from immune complex reactions after recovery from acute or subclinical disease
Infectious Canine Hepatitis – DIC • Disseminated Intravascular Coagulation – • A frequent complication of ICH • Begins in the early viremic phase of the disease • May be triggered by exposure of subendothelial collagen and subsequent platelet aggregation and/or inability of the damaged liver to remove activated clotting factors • Clinical Features – • IP – 4-9 days. • ICH is most frequently seen in dogs less than one year of age • Although unvaccinated dogs of all ages can be affected • Most infections are asymptomatic • In systemic infections there are 3 over-lapping syndromes which are usually seen in puppies less than 6 months of age • Peracute disease, acute disease and mild cases
Infectious Canine Hepatitis – Clinical Features • Peracute disease – dog found dead after illness lasts 3-4 hours. Due to massive destruction of hepatocytes • Acute disease – Dogs that survive the viremic phase • Fever, depression, vomiting, bloody diarrhea, petechial and echhymotic hemorrhages of the mucous membranes, pale mucous membranes, jaundice, DIC • Mild cases • Clinical signs in mild disease of ICH last 5-7 days prior to improvement • Encephalitis – Common in foxes (ischemia) – fox encephalitis – but less common in dogs
Infectious Canine Hepatitis – Diagnosis and Immunity • Diagnosis – Based on clinical signs, lab findings • Virus isolation in cell culture – URINE, blood, nasal secretions and tissues • Antigen detection in tissues – FAT, PCR • Paired sera – employs virus neutralization, ELISA, or hemagglutinination-inhibition tests • Gross and histopathology; hematology or leukopenia • Immunity – • Recovered animals are immune to the systemic form of the disease but may not resist an aerosol challenge and may develop respiratory disease • Maternal antibody interferes with active immunization until puppies are 9-12 weeks of age • Both inactivated virus and attenuated/modified virus CAV-1 vaccines are used • Annual revaccination is recommended • Modified live vaccine localizes in the kidney and causes a mild subclinical interstitial nephritis and a persistent shedding of virus - <1% of puppies may develop corneal edema • Attenuated CAV-2 vaccines provide cross-protection against CAV-1
Canine Infectious Tracheobronchitis – ITB – Kennel cough • Kennel cough is mostly self-limiting respiratory disease of dogs • Etiologic agents – CAV-2, Canine parainfluenza 2, Bordatella bronchiseptica, Mycoplasma cynos • Other contributing factors include – CAV-1 and Canine Morbillivirus (canine distemper) • Transmission – highly contagious – via aerosols • Clinical Features – IP – 30 days • Uncomplicated ITB • Mild respiratory disease – laryngitis, tonsilitis, pharyngitis, tracheitis, bronchitis • Paroxysms of dry, hacking, mostly nonproductive cough, followed by retching • Rhinitis with serous to mucopurulent nasal discharges
Canine Infectious Tracheobronchitis - ITB • Usually resolves in 2 weeks • Diagnosis – similar to CAV-1 • Palpation of trachea stimulates coughing attack • Immunity – CAV-2 vaccination –MLV is routinely incorporated into vaccine protocols recommended for all dogs
Equine Adenovirus Infections • Worldwide • Arabian foals in the USA since 1970 • Very susceptible due to combined T and B cell immunodeficiency • As maternal antibody wanes, the foals become increasingly susceptible due to their combined T and B cell immunodeficiency • Diseases associated with Aviadenoviruses – 12 serotypes • Species – • chicken – inclusion body hepatitis; egg drop syndrome 1976 • Ducks – Hepatitis – RARE • Quail – Bronchitis • Turkeys – Bronchitis – hemorrhagic enteritis; marble spleen disease