Download
1 / 36
460 likes | 2.7k Views
AGGRESSIVE PERIODONTITIS. INDEX. INTRODUCTION LOCALIZED AGGRESSIVE PERIODONTITIS Historical background Clinical features Radiographic findings Histopathologic features Bacteriology Immunology Treatment GENERALIZED AGGRESSIVE PERIODONTITIS Clinical characteristics

E N D
INDEX • INTRODUCTION • LOCALIZED AGGRESSIVE PERIODONTITIS • Historical background • Clinical features • Radiographic findings • Histopathologic features • Bacteriology • Immunology • Treatment • GENERALIZED AGGRESSIVE PERIODONTITIS • Clinical characteristics • Radiographic findings • Risk factors • CONCLUSION
INTRODUCTION DEFINITION Aggressive periodontitis is characterized by the rapid loss of attachment and bone loss occurring in an otherwise clinically healthy patient with the amount of microbial deposits inconsistent with disease severity and familial segregation of diseased individuals.
Localized aggressive periodontitis was formerly classified as early onset periodontitis and localized juvenile periodontitis (LJP) . • Generalized aggressive periodontitis was previously classified as generalized juvenile periodontitis (GJP) and rapidly progressive periodontitis (RPP).
LOCALIZED AGGRESSIVE PERIODONTITIS HISTORICAL BACKGROUND: • In 1923, Gottlieb reported a case of diffuse atrophy of alveolar bone characterized by the loss of collagen fibers in the periodontal ligament and loss of alveolar bone. • In 1928 Gottlieb attributed this condition to the inhibition of cementum formation and termed the disease as cementopathia.
In 1942, Orban and Werbmann introduced the term periodontosis and on the basis of autopsy cases described three stages in the development of the disease. • Stage 1: Involves the degeneration of principle fibers of the periodontal ligament, which induces cassation of cementum formation and resorption of alveolar bone. • Stage 2: The lack of periodontal fibers results in the rapid proliferation of the junctional epithelium along the root and earliest signs of inflammation appear. • Stage 3: It is characterized by progressive inflammation and the development of deep, infrabony periodontal pockets.
Most of the studies which followed considered ‘Periodontosis’as a degenerative disease caused by unknown systemic factors. • Other investigators observed the existence of a degenerative type of periodontal disease and attributed the changes observed to trauma from occlusion. • In 1996, the World Workshop concluded that “periodontosisas a degenerative entity was unsubstantiated and the term should be eliminated from periodontal nomenclature.” • The term juvenile periodontitis was introduced by Chaputand colleagues in 1967 and by Butler in 1969.
In 1971, Baer defined it as a disease of periodontium occurring in an other wise healthy adolescent which is characterized by a rapid loss of alveolar bone, about more than one tooth of the permanent dentition. The amount of destruction is not commensurate with the amounts of local irritants.
A more recent definition by Genco et al 1986 describes localized juvenile periodontitis as a disease occurring in otherwise healthy individuals order than 30 years of age with destructive periodontitis localized to the first permanent molars and incisors not involving more than two other teeth. • Generalized juvenile periodontitis is defined as destructive periodontitis in individuals under the age of 16 years affecting more then fourteen teeth i.e generalized to an arch or an entire dentition.
CLINICAL FEATURES AGE AND SEX DISTRIBUTION • Affects both the sexes and is seen mostly between puberty and 20 years of age. Some studies show predilection to female patients. DISTRIBUTION OF LESIONS: • Three areas of localization of bone loss have been described. • First molar and/or incisors. • First molar and/or incisors & additional teeth (not exceeding 14 teeth) • Generalized involvement
For localized juvenile periodontitis classic distribution is in the first molars and incisors with least destruction in the cuspid, premolar area. Limitations of destruction to certain teeth could be for the following reasons.
1) Production of opsonising antibodies against A. actinomycetemcomitins called “Burn out” phenomenon. 2) Bacteria antagonistic to A. actinomycetemcomitans may develop thereby decreasing the number of colonization sites. 3) A. actinomycetemcomitans may loose its leukotoxin producing ability for unknown reasons. 4) Localization of the lesions could also be due to the defect in cementum formation (hypoplastic/ aplastic cementum).
CLINICAL FINDINGS 1. The most striking feature is lack of clinical inflammation despite the presence of deep periodontal pockets. 2. There is a small amount of plaque, which forms a thin film on the tooth and readily mineralizes to become calculus. 3. Most common initial symptoms are mobility and migration of first molars and incisors. Classically, a distolabial migration of the maxillary incisors with diastema formation occurs. Lower incisors rarely migrate compared to upper incisors . All changes followed by sequelae of migration are seen. 4. As the disease progresses other symptoms like root surface sensitivity , deep dull radiating pain, periodontal abscess formation and regional lymphnode enlargement may occur.
CASE-1 AGGR.PDITIS CASE-2 CASE-2 AGGR.P’DITIS
RADIOGRAPHIC FINDINGS • Vertical or angular bone loss around the first molars and incisors in an otherwise healthy teenagers is a diagnostic sign of classical localized aggressive periodontitis. The pattern appears to be, ‘Arc shaped loss of alveolar bone extending from distal surface of 2nd premolar to mesial surface of 2nd molar’. • Frequently, bilaterally symmetrical patterns of bone loss occurs, called as a “mirror image pattern”.
Pathogenesis of aggressive periodontitis is due to an interplay of several factors like, • the specific microbiology of subgingival plaque • defects in cementum • hereditary factors • impaired PMNs functions • disorders of the immune system.
HISTOPATHOLOGY • Same as those seen during pocket formation like, • ulcerated pocket epithelium. • accumulation of various inflammatory cells in the connective tissue mainly leukocytes, plasma cells and small number of lymphocytes and macrophages. • Electron microscopic studies of juvenile predisposition revealed bacterial invasion of connective tissue that reaches the bone surface. • The flora involves A.actinomycetemcomitans,Capnocytophagasputigena and others.
BACTERIOLOGY • Two types of bacteria are considered to be pathogens in localized aggressive periodontitis- A. actinomycetemcomitans and Capnocytophaga sp. A. actinomycetemcomitans is a short, facultative anaerobe, non- motile, gram- negative rod.
Virulance factors associated with A. a Factors Significance. Leukotoxin Endotoxin Bacteriocin Collagenase Chemotacticinhibition factors • Destroys polymorphonuclear leukocytes and macrophages • Activates host cells to secrete inflammatory mediators (PG’s), interleukins and tumor necrosis factor – α • May inhibit IgG and IgM production • Causes degradation of collagen • May inhibit neutrophilchemotaxis.
IMMUNOLOGY • Immune defects that have been implicated in the pathogenesis of localized aggressive periodontitis are functional defects of polymorphonuclear leukocytes/ monocytes thereby impairing the chemotactic attraction of polymorphonuclear leukocytes to the site of infection.
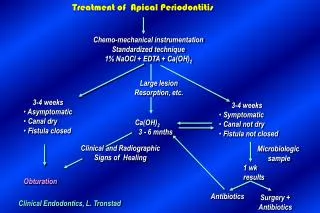
TREATMENT 1. Extraction: Extraction of involved teeth especially first molars results in uneventful healing. Transplantation of developing third molars into the sockets of previously extracted 1st molars has been tried but with limited success. 2. Standard periodontal therapy: Includes scaling, root planing, curettage, flap surgery with /without bone grafts, root amputation, hemisection, occlusaladjustment and strict plaque control . However response is unpredictable and frequent maintenance visits are mandatory. 3. Antibiotic therapy: several authors reported successful results using antibiotics as an adjunct to standard therapy. • Genco and coworkers reported scaling and root planingand tetracycline 250mg qidfor 14 days every 8 weeks. • Several other investigators have also noticed excellent bone fill in cases of localized juvenile periodontitis treated with tetracycline, flap surgery and placement of grafts.
MANAGEMENT AGGR.P’DITIS FLAP SURGERY
CURRENT APPROACH TO THERAPY • In almost all cases systemic tetracycline hydrochloride 250mg qid for atleasta week should be given in conjunction with local mechanical therapy. If surgery is indicated systemic antibiotics are advised with patient instructed to start the antibiotic approximately 1 hour before surgery. • Doxycycline loading dose of 200 mg on 1st day followed by 100mg/day for 6 days may also be used. • Chlorhexidine rinses should be prescribed. • In refractory cases, tetracycline resistant Actinobacillus species have been suspected. In such cases combination of amoxicillin and metronidazolehas been suggested.
GENERALIZED AGGRESSIVE PERIODONTITIS • Generalized aggressive periodontitis (GAP) is usually characterized by generalized interproximal attachment loss affecting atleast three permanent teeth other than first molars and incisors. Patients with GAP form may exhibit minimal amounts of microbial plaque associated with the affected teeth. • Quantitatively, the amount of plaque seems to be inconsistent with the amount of periodontal destruction. • Qualitatively most pathogenic organisms may be associated. Eg: Porphyromonas gingivalis, A.actinomycetemcomitans and Bacteroides forsythus.
CLINICAL CHARACTERISTICS Age and sex distribution: It affects persons between puberty and 35 years (but may be older) .No sex discrimination is seen. Distribution of lesion:No specific pattern is observed, all or most of the teeth are affected. • Two types of gingival responses may be seen in GAPeriodontitis. • One is severely, acutely inflamed tissue which is often showing proliferation , ulceration ,fiery red colour , spontaneous bleeding, and suppuration . • In other cases, the gingival tissue may appear pink and free of inflammation but deep pockets can be demonstrated by probing. • Some of the patients may have systemic manifestations such as weight loss, mental depression and general malaise.
RADIOGRAPHIC FINDINGS • No definite pattern of distribution occurs but, the radiographic picture can range from severe bone loss associated with the minimal number of teeth, to advance bone loss affecting the majority of teeth in the dentition.
RISK FACTORS FOR AGGRESSIVE PERIODONTITIS • MICROBIOLOGIC FACTORS • IMMUNOLOGIC FACTORS • GENETIC FACTORS • ENVIRONMENTAL FACTORS
MICROBIOLOGIC FACTORS: • A. actinomycetemcomitans has been implicated as the primary pathogen associated with this disease. Microscopically, the lesions of localized aggressive periodontitis have revealed bacterial invasion of connective tissue that reaches the bone surface. These invading bacteria which have been identified are A. actinomycetemcomitans, Capnocytophaga sputigena, Mycoplasma sub- species and Spirochetes.
IMMUNOLOGIC FACTORS • Some of the immune defects that have been implicated in the pathogenesis of localized aggressive periodontitis(LAP) are: • Approximately 75 percent of patients with LAP have dysfunctional neutrophils, which express a decrease in the chemotactic response to several chemotactic agents like the complement component C5a, N- formyl– methionylleucylphenylalanine (FMLP) and leukotriene B4. The defect is also associated with a 40 percent deficiency in glycoprotein, GP110, on the neutrophil surface.
b)Patients with LAP demonstrate a strong antibody response to A. actinomycetemcomitans which explains the limitation of the infection. In LAP the dominant serum antibody is IgG2 type which is specific to antigens of A.actinomycetemcomitans. c) In generalized form of aggressive periodontitis disease microbial patterns including organisms associated with chronic periodontitis have been implicated. Host response is often characterized by defect in either neutrophils or monocytes.
GENETIC FACTORS • Some of the above mentioned immunologic defects seen in aggressive periodontitis may have a genetic basis, i.e, familial clustering of neutrophil abnormalities may be seen. It has been suggested by some authors that, a major gene plays a role in aggressive periodontal disease, which could be transmitted through an autosomal dominant mode of inheritance.
ENVIRONMENTAL FACTORS • Smoking is one of the factors that can influence the extent of destruction seen in young patients. Especially, smokers with generalized aggressive periodontitis exhibit more number of teeth affected by loss of clinical attachment than non- smokers with generalized aggressive periodontitis.
CONCLUSION • Aggressive periodontitis generally affects systemically healthy individuals less than 30 years old, although patients may be older. Aggressive periodontitis may be universally distinguished from chronic periodontitis by the age of onset, the rapid rate of disease progression, the nature and composition of associated flora, alterations in the host’s immune response and a familial aggregation of diseased individuals. In addition, a strong racial influence is observed in the United States, the disease is most prevalent among African Americans.