Download
1 / 29
290 likes | 417 Views
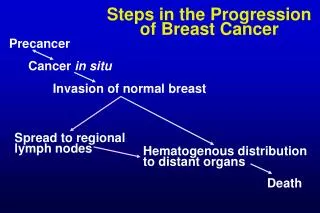
Aim . A randomized controlled trial to determine if an intensive program of Breast Self Examination (BSE) instruction would reduce mortality from breast cancer was carried out in Shanghai from October 1989 to December 2000.The trial involved 266 064 women permanent residents, born between 1925 to 1

E N D
1. Thomas DB et. al. Randomized Trial of Breast Self-Examination in Shanghai: Final Results. Journal of the National Cancer Institute 2002;94:1445-57
Presenter: Joe Lau
Mentor: David Thomson
2. Aim A randomized controlled trial to determine if an intensive program of Breast Self Examination (BSE) instruction would reduce mortality from breast cancer was carried out in Shanghai from October 1989 to December 2000.
The trial involved 266 064 women permanent residents, born between 1925 to 1958, who were either current or retired employees of the Shanghai Textile Industry Bureau (STIB)
3. Setting Primary medical care was from factory clinics, care beyond that was received from 1 of 3 hospitals operated by the STIB or to other hospitals having contracts with individual factories
There was no mammography available
Retired workers committees in individual factories maintained regular contact with retirees, being responsible for their housing and pension.
4. Methods - Recruitment Field operations were conducted by 34 specially trained former factory workers (BSE workers) and 5000 factory medical workers.
Study instruments and protocols were initially pilot tested and modified before the trial in pilot factories
519 factories were stratified according to size and hospital affiliation then randomly allocated to either BSE or control groups
Eligible women were identified from factory records and entered into a computer database in 1988
Medical workers then administered a questionnaire to all eligible women between 1989 � 1991 which included questions on risk factors and history of previous breast cancer
5. Methods - Numbers of recruited women
6. Methods BSE Instruction / Reinforcement Initial session (October 1989�October 1991) was at time of questionnaire where BSE workers taught a 3 step BSE technique to groups of 10 women and gave information about breast cancer and normal breast anatomy. It ended with individual instruction.
Video Reinforcement Sessions � In groups of 10, 1 and 3 years after initial instruction followed by individual supervised BSE practice.
Supervised practice sessions � 1,3,6 and 9 months after initial instruction for current workers and 1 and 6 months after for retired workers. Then every 6 months from year 2 to year 5.
Other reminders � posters, factory broadcasts, letters, reminders at meetings held for other purposes and home visits
Women in control group received no instruction but sessions on prevention of low back pain were held concurrently with 2nd video session
7. Methods - Proficiency Testing 10 BSE and 10 control factories were randomly selected before, immediately after and 1 year after each of the 2 video sessions, with the exception that only 5 in each group were selected after the 1st session.
25 current and 25 retired workers randomly selected per factory and on their ability to detect lumps of varying sizes in 3 breast models randomly chosen from a set of 6
Technique and coverage was recorded on standardized forms
8. Methods - Cohort Follow Up There was strict follow up with BSE workers visiting factory clinics, payroll offices and retirement committee offices to enquire about deaths every 1-2 months
Factory medical workers reported deaths, transfers and retirements in their own factories on standardized forms
Deaths were also reported to the STIB Tumor and Death registry as an annual summary
Reinforcement sessions also used for follow up
Data of women in trial periodically checked and updated. Only 7.5% of women (equally distributed between both groups) severed ties with their factories.
9. Methods - Case Finding Suspicious lumps reported to medical workers were referred to surgeons
Further investigation and management did not involve study personnel
Information on identity, detection and treatment was transferred to standardized forms. This information was supplemented by regular BSE worker visits to hospitals, reviews of annual summaries received by the STIB Tumor and Death registry and the Shanghai Cancer Registry.
Efficiency of methods tested by comparing study detection rates with expected rates derived from the Shanghai Cancer Registry. Standardized Incidence Ratio 1.12 (95 % CI 1.06 to 1.19)
10. Methods- Diagnostic Confirmation Medical records reviewed and lumps recorded as being benign or malignant. Histological diagnosis and TNM stage also were recorded
Slides of sections reviewed by local pathologist and sent to Seattle for storage and review by reference pathologist.
10/1044 slides of breast cancer that were reviewed were not confirmed as breast cancer
17/1071 slides of benign lesions reviewed found to contain evidence of breast cancer
Estimated 29 and 19 cancers in the BSE and control group respectively were missed
11. Methods - Deaths from Breast Cancer All women with cancer or benign breast disease were actively followed up, by home visits if necessary
Reports of all deaths from breast cancer were also obtained from the STIB Tumor and Death Registry
Clinical records of each death reviewed by a physician who interviewed friends and family if necessary to determine if breast cancer was the cause of death
Summary of information and cause of death as being very likely, probably, probably not or very likely not due to breast cancer were recorded
12. Data Processing and Analysis All judgment regarding diagnosis and coding of lesions/cause of death/inclusion or exclusion of women during data processing were made without knowledge of the study arm
Women in certain areas/factories might have similar risk factors or medical care that could influence breast cancer incidence or mortality
Variations in incidence noted at preliminary analysis was completely accounted for by stratification on hospital of affiliation
Thus randomization of factories was stratified on hospital of affiliation
13. Data Processing and Analysis Mortality rates estimated using standard life table methods with time measured from date of entry
Women censored from the analysis at the time they left STIB/were lost to follow-up/ or at time of death from other causes
Survival was calculated from time of entry into study and from time of diagnosis to death
Survival probabilities were estimated using life table and Kaplan-Meir methods
Differences between survival were evaluated using the log-rank test and cumulative risk ratios estimated using Cox proportional hazards models
14. Results
15. Results - Compliance 80% of women attended all 3 sessions (instruction, 1st and 2nd video sessions)
Total number of initial instruction, reinforced and supervised BSE sessions for current workers was 15 and 13 for retired workers with the mean and median sessions attended being 12.3 and 13 for current workers and 11.1, 12 for retired workers
Only 10% in both groups attended <8 sessions
16. Results - Proficiency Women were tested immediately before and after and 1 year after video sessions
Instruction group performed better than the control group in all settings, proficiency improved immediately after video session but then dropped back to pre-video level 1 year later
Women in control groups were more specific
Similarly technique and coverage improved straight after the 1st video but declined back to pre-video levels a year later
18. Results - Intermediate Variables Slightly more women in the control group were diagnosed with breast cancer but the difference is not statistically significant (p =.47)
More benign breast disease was detected in the BSE group
More women in the BSE group had biopsies
19. Apart from 1st 6 months, where there was a large difference in the number of histologically diagnosed cancers (likely prevalent pre-existing) the numbers diagnosed were similar between both groups
Statistically significantly more women in the BSE group had benign lesions diagnosed (p <.001) and these lesions tended to be slightly smaller
Biopsy:cancer ratio 4.2 in BSE group compared to 2.7 in the control
Slightly higher percentage of cancers were diagnosed in the in-situ/T1 stage in the instruction group but this was not statistically significant p=0.60
20. Results - Intermediate Variables A slightly higher percentage of women who had attended all instruction sessions were diagnosed at Tis or T1 than those who attended fewer sessions 52.3% (56 of 107 current workers) compared with 45.3% (78 of 172) who attended <11 sessions. P=.67. A similar difference was observed in retired women but this was also not statistically significant P=.97
There were no differences in the number of women with nodal involvement between the 2 groups, in total or by stage
21. Results - Detection and Treatment 81.9% of women in the BSE group found their breast cancer while practicing BSE
96.4% of women in the control group found the cancers �by themselves� or �accidentally�
Time from detection to evaluation was slightly more prompt in the instruction group with 65% evaluated within a week compared to 58.7%
Time from referral to treatment was the same, with a median of 14 and 13 days (p=.48) in BSE and control groups respectively
22. Results - Treatment
P=.06
Stratification by stage revealed that difference in women with breast conserving surgery was not because tumors were detected at earlier stage
Equal proportions of women in both groups received radiation, hormonal, chemotherapy or combinations
93.8% of women in both groups received systemic therapy with hormones / chemotherapy or both
23. Results - Mortality Survival in the 2 groups was 95.2% (CI = 95.1 to 95.3) and 94.9% (CI = 94.7 to 95) in the BSE and control groups respectively
154 (0.12%) in the BSE group and 158 (0.12%) in the control group developed breast cancer and died
Likelihood of death being due to breast cancer:-
Differences not statistically significant (p=.67)
0.1% (135 & 131) � very likely/probably died from cancer
24. Results - Mortality Cumulative mortality rates for years after entry into trial are similar (150.6 versus 120.6 per 100,000 women years, p=.72)
Cumulative risk ratio for women in BSE group to women in control group 1.04 with 95% CI 0.82 � 1.33
Cumulative risk ratios based on deaths from breast cancer were 1.23 (95% CI 0.83 to 1.82) and 0.96 (95% CI 0.7 to 1.31) in women under and over 50 years of age respectively
25. Results - Survival
26. Discussion This trial did not show a reduction in mortality from a massive effort to teach and encourage women to perform BSE. Study had a 80% power to detect a true reduction in risk of about 30% (level of risk reduction observed in mammography)
Despite slightly higher numbers of women in the BSE group finding lesions that were smaller or in-situ and seeking medical attention slightly more promptly, as many cancers in the instruction group had nodal disease at diagnosis. Tumors were not diagnosed any earlier and survival time from diagnosis was similar between the 2 groups.
These results are unlikely due to inadequate duration of study as randomized trials of mammography in women show a reduction in breast cancer mortality rates after about 5 years of follow up 1
Another randomized controlled trial in St. Petersburg Russia involving 120,000 women also did not show improved mortality rates in women taught BSE2
27. Discussion Possible sources of bias-
There was 3 times as many exclusions from the BSE (2.6%) group compared to the control group (1.0%), likely because the BSE group were asked to make a bigger commitment. It is virtually impossible that the mortality rates in the excluded women could have been so extreme as to alter the overall mortality rates however.
Variation of incidence among factories noted at baseline completely accounted for by stratification by hospital of affiliation. They corrected for this by randomization after stratification by hospital affiliation
In 1994, China shifted to a market economy leading to some factory closures and merges. Factory wide activities of the larger of the 2 factories were continued after merging but all women were retained in original study arm. In total only 5725 (4.3%) transferred from BSE to control group and 4783 (3.6% vice versa) within 5 years of entering into study (reinforcement activities ceased after 5 years)
Only 7.5% of women severed their ties to the factory and this was the percentage for both groups, thus it is unlikely that loss of these women to the full follow up could account for trial outcome.
More woman died in the control group compared to the BSE group 5939 (4.5%) compared to 5349 (4%). There were no obvious differences in specific causes of death that contributed disproportionately to the overall differences in mortality rates. However, this difference might reflect an under-ascertainment of deaths in the BSE group, which would make BSE seem more efficacious rather than mask a true beneficial effect.
It was estimated that 35 cancers were missed, however these would have been evenly distributed between the 2 groups and even in the unlikely scenario that half of the missed cancers in the control group died while all in the BSE group survived, this would only mean an additional 9 cancer deaths and the relative risk would still be 1.
28. Discussion Frequency of women performing BSE outside of supervision is unknown, although BSE was practiced a minimum every 5 months for 4-5 years in this trial
Other observational studies have shown tumor size to be inversely proportionate to frequency of BSE practice3,4 suggesting that it could be possible for motivated women to be taught to detect cancers that develop between regular screenings.
A randomized trial in which all women receive mammograms and half received instruction in BSE would be helpful.
The universality of the findings in this study is questionable, as cultural context and associated values and behaviors were ignored. Other studies have shown difference in behaviors and attitudes in Asian women toward breast education and screening5,6,7
29. References 1. Nystrom L. et al Breast cancer screening with mammography : overview of Swedish randomised trials. Lancet 1993;342:1372
2. Semiglazov VF et al. Interim results of a prospective randomized study of self-examination for early detection of breast cancer. Vopr Onkol 1999;45(3):265-71
3. Feldman JG et al. Breast self-examination, relationship to stage of breast cancer at diagnosis. Cancer 1981;47:2740-5
4. Tamburini M et al. Usefulness of breast self-examination for an early detection of breast cancer. Results of a study on 500 breast cancer patients and 652 controls. Tumori 1981;67:219-24
5. Sadler Gm et al. Chinese women:behaviors and attitudes toward breast cancer education and screening. Womens Health Issues 2000; 10:20-26
6. Tang TS et al. Cultural barriers to mammography, clinical breast exam and breast self exam among Chinese-American women 60 and older. Prev Med 2000; 31:575-583
7. Straghan PT et al. Attitudes as barriers in breast screening: a prospective study among Singapore women. Soc Sci Med 2000; 51: 1695-1703.