Download
1 / 73
730 likes | 781 Views
Learn about the assessment, treatment, and transfer criteria for burn injuries, as well as the pathophysiology, clinical features, and management of carbon monoxide poisoning.

E N D
Emergency Medicine Special Situations:BurnsCarbon MonoxideElectrical InjuriesLightning Thomas Vu Resident Weekly Conference 08/07/2019
Burns • Overview • Size • Depth • Inhalational Injury • Wound Care • Escharotomies • Transfer Criteria • Minor burns
Burns - Overview • 450,000 people/year seek medical treatment for burns • 40,000 people require hospitalization • 60% of those treated at burn center; 4% those treated in burn centers die • ***Otherwise, vast majority treated acutely in ED
Burns - Overview • Skin functions to • Prevent water loss • Protects against environmental assault • Aids in body temp control/sensation/excretion • Effects of thermal burns • Intracellular influx Na/Water, efflux K • Myocardial depression • Systemic vascular resistance • Metabolic acidosis • Release of histamines, kinins, serotonins, free oxygen radicals • Local tissue injury • Hematologic changes
Burns - Inhalational • Most fire-related deaths are due to smoke inhalation • Produces mucosal edema of airway, decreases alveolar surfactant activity, bronchospasm, ARDS (50% of intubated burn patients) • Facial burns, singed nasal hair, soot in mouth or nose, hoarseness, carbonaceous sputum, expiratory wheezing • Carbon monoxide, Cyanide exposure
Burns - Inhalational *****Indications to intubate: ***** 1) Full thickness burns of face/perioral region 2) Circumferential neck burns 3) ARDS 4) Progressive hoarseness/air hunger 5) Respiratory depression or AMS 6) Supraglottic edema and inflammation on bronchospasm 7) Anticipated clinical course
Burns – Wound Care • Initially – cover with dry, clean sheet • Later small burns cover with moist saline dressing • Large burns cover with sterile drapes (avoid hypothermia) • Likely avoid antiseptic dressing in ED • Allow for admitting/transfer facility to assess wound
Burns - Escharotomies • Limbs may develop compromise, especially after initiation of resuscitation • Check pulses, cap refill, pulse ox, skin temp, doppler flow • Escharotomy indicated if vascular compromise is evident • Incise with scalp to level of fat on mid-lateral portion of limb, avoid fascia; extend to hand/fingers
Burns - Escharotomies • Escharotomy of chest wall to allow for adequate ventilation if circumferential burns of chest and neck • Incise at both anterior axillary lines from level of second rib to twelfth rib • Join these two incisions transversely
Burns – Burn Center Transfer Also consider • Partial thickness >25% BSA (10-50y) • Partial thickness >20% BSA (<10, >50) • Burns involving face, eyes, ears, genitalia, joints, hands, feet • Circumferential burns of an extremity Can consider hospitalization without transfer • Partial thickness 15-25% BSA (10-50y) • Partial thick 10-20% BSA (<10, >50) • Full thickness burns <10% in anyone
Silvadine may interfere with partial thickness healing, offers no healing advantage (inhibits keratinocytes)
Burns – Minor Burns • Don’t forget tetanus & analgesics
Carbon Monoxide • Overview • Pathophysiology • Clinical Features • Diagnosis • Treatment
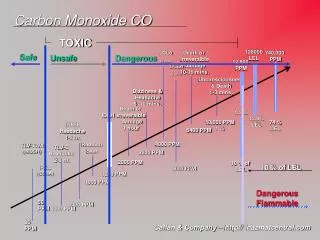
Carbon Monoxide - Overview • Most common cause of fatal poisoning (suicidal or accidental) • Great deal of controversy about approach • CDC – estimates 430 deaths/year • CO detectors has not decreased deaths
Carbon Monoxide - Pathophysiology • Binds to hemoglobin – 200x stronger affinity than oxygen • Forms Carboxyhemoglobin • Half life • Room Air= 249-320 min • 100% O2 = 74-80 min • Causes relative anemia, shifts O2 dissociation curve to left • Intracellular effects: uncouples oxidative phosphorylation, enzymatic hypotension, neutraphilic inflammatory response
Carbon Monoxide – Clinical Features • Should consider in differential of patients comatosed, mental status changes, unexplained AG elevation or lactic acidosis
Carbon Monoxide - Diagnosis • Co-oximetry – measures oxy-hgb, met-hgb, co-hgb • Most accureate measuring tool • Arterial and venous blood gas carboxyhemoglobin • ABG vs VBG similar values • Symptoms and levels do not always correlate • Other tests – lactic acid, AG, CPK, EKG
Carbon Monoxide - Treatment • ABCs as usual • 100% O2 on NRB if symptomatic • Hyperbaric Oxygen when indicated • Half life • Room Air= 249-320 min • 100% O2 = 74-80 min • How long does it take to transfer someone? …so why transfer someone??? Decreases severity/incidence of delayed neurologic sequelae
Carbon Monoxide - Treatment • ABCs as usual • 100% O2 on NRB if symptomatic • Hyperbaric Oxygen when indicated • Half life • Room Air= 249-320 min • 100% O2 = 74-80 min • How long does it take to transfer someone? …so why transfer someone??? Decreases severity/incidence of delayed neurologic sequelae
Carbon Monoxide - Treatment • ABCs as usual • 100% O2 on NRB if symptomatic • Hyperbaric Oxygen when indicated • Half life • Room Air= 249-320 min • 100% O2 = 74-80 min • How long does it take to transfer someone? …so why transfer someone??? Decreases severity/incidence of delayed neurologic sequelae
Carbon Monoxide - Treatment • ABCs as usual • 100% O2 on NRB if symptomatic • Hyperbaric Oxygen when indicated • Half life • Room Air= 249-320 min • 100% O2 = 74-80 min • How long does it take to transfer someone? …so why transfer someone??? ****Decreases severity/incidence of delayed neurologic sequelae
Carbon Monoxide - Treatment • ABCs as usual • Always consider cyanide toxicity for a critically ill, unstable patient from a fire
Carbon Monoxide - Treatment Disposition • Min intox, mild symptoms – can d/c after period of observation (if not suicidal) • Transfer those indicated for HBO or high clinical concern after consultation with HBO specalist
Electrical Injuries • Overview /Physics Basics • Clinical Features • Pre-hospital Care • ED Care
Electrical Injuries – Overview/Physics Basics • 6,500 electrical injuries per year • 61% work releated • 1800 work place fatalities between 2003-2019 • High-voltage high morbidity • Deep-muscle necrosis often needing fasciotomy, amputation
Electrical Injuries – Overview/Physics Basics • 6,500 electrical injuries per year • 61% work releated • 1800 work place fatalities between 2003-2019 • High-voltage high morbidity • Deep-muscle necrosis often needing fasciotomy, amputation