Download
1 / 99
1.01k likes | 1.26k Views
Pharmacological and Parenteral Therapies. Dena Evans, MPH, BSN, RN Assistant Professor Department of Nursing The University of North Carolina at Pembroke. Aminoglycosides. What are they? Give examples What do they treat specifically? Toxicity Labs associated Routes of administration.

E N D
Pharmacological and Parenteral Therapies Dena Evans, MPH, BSN, RN Assistant Professor Department of Nursing The University of North Carolina at Pembroke
Aminoglycosides • What are they? • Give examples • What do they treat specifically? • Toxicity • Labs associated • Routes of administration
Answers • They are bacteriocidal antibiotics • Amikacin; gentamicin; neomycin; streptomycin • Gram negative bacteria like pseudomonas, enterobacter and TB
Toxicity • Dose related • Given based on client’s weight • Can cause ototoxicity and nephrotoxicity • Why: ½ life in renal cortex is 100 hours so------
Labs • What labs should we monitor and why?
Normal Creatinine • 0.6 to 1.3 mg/dL
Drug Interactions • Cephalosporins (Keflex; Ceclor) increase the risk of nephrotoxicity • Loop diuretics (Lasix) increase the risk of ototoxicity
Questions • The nurse is reviewing the client’s record and notes that the physician has documented that the client has a renal disorder. On review of the laboratory results, the nurse would most likely expect to see which of the following: a. Decreased hgb b. Elevated creatinine c. Decreased RBCs d. Decreased WBCs
Dosage Calculation Based on Weight • The MD orders Gentamycin 50mg/kg/day and the recommended dosage is 200-500 mg/kg/day. Your patient weighs 10 kg. • Question 1: How many mg has the MD ordered? • Question 2: Is the dosage safe: • Question 3: How do you know if it is safe?
Dosage Calculation Tobramycin • The physician order tobramycin 15mg IV q 6h for a child with a severe systemic infection who weighs 10kg. You have on hand 20mg/2mL. Recommended pediatric parameters are 6-7.5 mg/kg/day in four divided doses. • Question 1: How many mL will you give? • Question 2: Is the order safe? • Question 3: How do you know?
Drug Question-Kidney • Following kidney transplantation, cyclosporine is prescribed for a patient. Which lab result would indicate an adverse effect from the use of this medication? • Decreased creatinine level • Decreased hemoglobin level • Elevated blood urea nitrogen level • Decreased white blood cell count
Drug Question-Kidney • Following kidney transplantation, cyclosporine is prescribed for a patient. Which lab result would indicate an adverse effect from the use of this medication? • Decreased creatinine level • Decreased hemoglobin level • Elevated blood urea nitrogen level • Decreased white blood cell count Indicates nephrotoxicity
Drug Therapy-Kidney • A client with chronic renal failure is receiving epoetin alfa (Epogen, Procrit). Which lab result would indicate a therapeutic effect of the medication? a. Hematocrit of 32% b. Platelet count of 400,000 cells/mm3 c. BUN of 15mg/dL d. WBC of 6,000 cells/mm3
Drug Therapy-Kidney • A client with chronic renal failure is receiving epoetin alfa (Epogen, Procrit). Which lab result would indicate a therapeutic effect of the medication? a. Hematocrit of 32% b. Platelet count of 400,000 cells/mm3 c. BUN of 15mg/dL d. WBC of 6,000 cells/mm3 This is the intended effect of the drug
Drug Therapy-Steroids • Prednisone is prescribed for a client with diabetes mellitus who is taking daily NPH insulin. Which of the following medication changes would the nurse anticipate during therapy with prednisone: a. An additional daily prednisone dose b. A decreased amount of daily NPH c. An increased amount of daily NPH d. The addition of an oral hypoglycemic agent
Drug Therapy-Steroids • Prednisone is prescribed for a client with diabetes mellitus who is taking daily NPH insulin. Which of the following medication changes would the nurse anticipate during therapy with prednisone: a. An additional daily prednisone dose b. A decreased amount of daily NPH c. An increased amount of daily NPH d. The addition of an oral hypoglycemic agent Steroids can trigger diabetes and worsen in existing cases
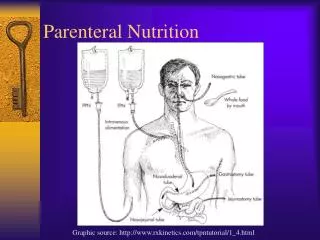
TPN Total Parenteral Nutrition
What is it? • Mixture • Specifically designed—individualized • Sugar, carbs, protein, lipids, electrolytes, trace elements • Should be clear—no sediment
Why would someone need it? • Can’t eat • Needs nutritional support • Cancer patient; transplant patient; stabilization of electrolytes in the elderly
Electrolytes--revisited • Sodium • Potassium • Chloride • Phosphate • Calcium • Magnesium
Question • Does having too much or too little of any electrolyte have the potential to cause health problems? • Give me an example
So… • If you have a patient who is already nutritionally challenged and you are giving them a solution of electrolytes via a central line, what signs and symptoms would you observe for?
Possibilities • Could you see an EKG changes? Why? What specifically? • Could you see issues with muscle strength? Why? What specifically? • Could you see an problems with mental status? Why? What specifically?
EKG Changes • Hyperkalemia may cause spiked “T” waves
Muscles • Hypocalcemia • Chvostek’s Sign • Trousseau’s www.sohnurse.com
Mental Status • Hypomagnesemia • Psychotic behavior/sedation/confusion
Side Effects of TPN • Mouth sores; skin changes; *fever, chills, stomach pain, *SOB, rapid wt. loss or gain; muscle weakness or twitching, jumpy reflexes, swelling of hands or feet • What type of patient do you think TPN should be use cautiously with?
Answer • Renal • Cardiac Insufficiency • Diabetics • Remember: Fluid overload (report SOB/ rapid wt. gain/swelling of hands and feet). • Hypokalemia: ESRD and poor nutrition coupled with extra fluid, sodium, potassium. • And TPN has a lot of sugar in it
What labs will you monitor? • Electrolytes • Kidney specific • ?Infection at site of central line? WBCs • Blood sugar due to high amounts of sugar in the mixture
Storage • Should be kept in fridge or freezer • Remove 4-6 hours before giving (why)? • Do not refreeze
TPN Question • A patient with Chron’s disease is receiving TPN via a subclavian triple lumen catheter. The nurse recognizes that a priority is to: • Assess the insertion site for signs of infection • Complete the administration within 8 hours • Discontinue the infusion if the patient experiences hyperglycemia • Change the IV tubing and dressing every 72 hrs. Coonan, P.R. (2006). NCLEX for dummies.
TPN Question • A patient with Chron’s disease is receiving TPN via a subclavian triple lumen catheter. The nurse recognizes that a priority is to: • Assess the insertion site for signs of infection • Complete the administration within 8 hours • Discontinue the infusion if the patient experiences hyperglycemia • Change the IV tubing and dressing every 72 hrs. Coonan, P.R. (2006). NCLEX for dummies.
Rationale • Infection is a major concern for clients receiving TPN • Usually given continuous drip • Never stop abruptly (hyPOglycemia • Change bag each time and dsg. Per policy
TPN Question • When caring for a patient who is receiving TPN, what should the nurse do to prevent infection in the patient? a. Encourage the patient to take fluids by mouth each day b. Monitor the serum blood urea nitrogen and blood sugar daily c. Maintain strict I&O records d. Use strict aseptic technique when caring for the IV site
TPN Question • When caring for a patient who is receiving TPN, what should the nurse do to prevent infection in the patient? a. Encourage the patient to take fluids by mouth each day b. Monitor the serum blood urea nitrogen and blood sugar daily c. Maintain strict I&O records d. Use strict aseptic technique when caring for the IV site
TPN Question • A patient is started on TPN. Which of the following lab tests should the nurse monitor several times a day? a. Serum calcium and magnesium b. Urine specific gravity c. Blood glucose d. Serum total protein
TPN Question • A patient is started on TPN. Which of the following lab tests should the nurse monitor several times a day? a. Serum calcium and magnesium b. Urine specific gravity c. Blood glucose d. Serum total protein
Questions • What is Clostridium Difficile? • Where is it found? • What is Rocephin? • What is it used for?
Answers • Clostridium Difficile is a resident flora of your intestinal tract. • It is not the most abundant flora • Rocephin is a broad-spectrum antibiotic. • What does that mean?
Rocephin and C-Diff • Give broad spectrum antibiotics—potentially wipe out good bacteria that keep flora in check (C-Diff). • This allows C-Diff, usually a minority bacteria, to multiply. • Causes pseudomembranous enter colitis.
What is that? • Condition marked by diarrhea, abdominal pain and foul smelling stool. • AKA: Antibiotic-Associated colitis
Question • How do you diagnose pseudomembranous entercolitis?
Question • How do you think you would treat C-Diff?
Treatment • Stop the broad spectrum antibiotics • Give Flagyl or Vancomycin
Long term use of Steroids Side Effects
Questions • What are steroids commonly used to treat? • What hormone do they mimic? • Where does this hormone come from? • What does this hormone do?
Answers • Anti-inflammatory • COPD; Asthma; Infections • Mimic cortisol • Comes from the adrenal cortex • Cortisol helps body cope during times of stress: illness/surgery/infection • Also triggers insulin release