Download
1 / 35
390 likes | 1.2k Views
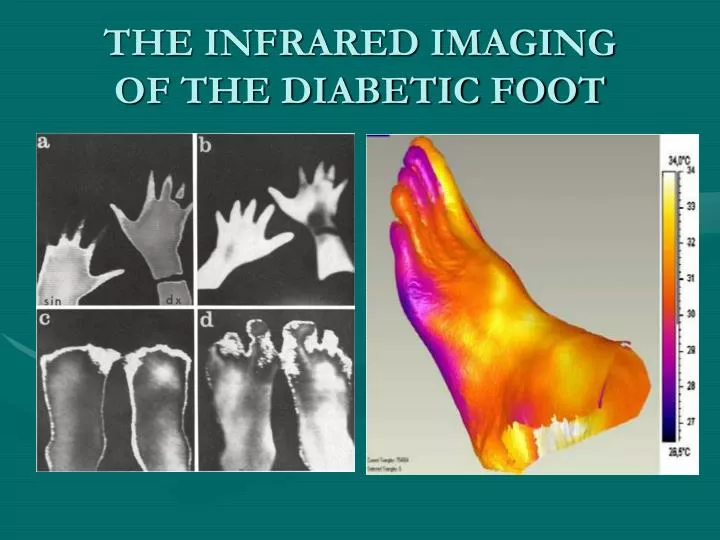
THE INFRARED IMAGING OF THE DIABETIC FOOT. A LITTLE HISTORY Infrared Thermography in Diabetes Mellitus P.I.Branemark, S.E.Fagerberg, L.Langer and Save –Soderbergh, Diabetologia 3, 1967 16 diabetics, 12 women and 4 man, mean age 28, average disease length 13 years.

E N D
A LITTLE HISTORY • Infrared Thermography in Diabetes Mellitus • P.I.Branemark, S.E.Fagerberg, L.Langer and Save –Soderbergh, Diabetologia 3, 196716 diabetics, 12 women and 4 man, mean age 28, average disease length 13 years
The emission over toes and metatarso-phalangeal regions was distinctly decreased and gave a sharp transverse boundary. Little or no reduction of the emission was shown over the dorsum of the foot and tibia. Asymmetric patterns were recorded from the only diabetic with local gangrene.
Disturbances in the arterial circulation • Detection of areas at high risk for ulceration or re-ulceration • Assessment of tissues viability, amputation level, and the intra-operative skin flap viability • Diagnosis of osteomyelitis • Evaluation of the medical treatment effectiveness • Assessment of microangiopathy and others vascular changes caused by the neuropathy
The examination of the diabetic foot • Room temperature : 24 C • Acclimatization time: 20 minutes • Undressed legs • Position : Orthostatism or seated with the lowers extremities hanging freely
The images are taken at fixed camera/object distances from the both legs in the anterior view, the foot from a top view and the soles • Hot spot is defined as an area at least 0,5 C warmer than surroundings • The thermal gradient represents the difference between the skin temperature at the knee and at the dorsum of the foot. • Thermal imaging of skin changes on the feet of type II diabetics – K.Ammer, P. Melnizky, O.Rathkolb, E.F. Ring- 2001 – 23rd Annual EMBS International Conference
Changes in the arterial circulation • Eco-Doppler • Angiography • Thermography
The “macro-circulation” pathology localizes more often below the popliteal fossa, than at the level of the aorta or iliac vessels • The injuries respect the distal (pedal) arteries • The changes are usually asymmetric, the tibial – peroneal triangle being the most commonly affected.
Thermography is especially useful to differentiate between “ischemic foot”(cold) and the “neuropathic foot(warm). • Detecting areas of critical ischemia
ARTERYOGRAPHY • Severe atheromatosis affecting the entire length of the tibial-peroneal trunk
ULCERATION • Neuropathic ( 40%) • Neuro-ischemic • Ischemic ( 10%)
It was suggested that examining thermographic patterns, patients with diabetis could be screened for risk of ulceration and that high temperature were predictive of ulceration. • In patients with diabetes peripheral neuropathies, and no additional pathology, the temperature of the right and the left lower extremities were not different.
Infrared dermal thermometry for the High-Risk diabetic foot • D.Armstrong, L.Lavery, P.Liswood, W.Todd, J.Tredweell-Physical Therapy, 77, 2, february 1997 • All patients who experienced ulceration or re - • ulceration during the follow-up period showed elevated skin temperature gradients.
The patients can be monitored to prevent ulcerations, higher temperatures having a predictive role for ulceration or re-ulceration (20- 58% of patients develop another ulcer within one year) • We have to keep in mind that the increased temperature indicates there is a problem and where it is, NOT WHAT IT IS !
The temperature monitoring is also recommended in patients with Charcot’s fractures, in the post-acute phase, after the inflammation had subsided. • Thermography is also useful in detecting subtle temperature changes that may persist in the post acute phase; a premature reactivation indicating reoccurrence.
OSTEOMYELITIS • Infrared imaging is a sensitive indicator of the presence or absence of osteomyelitis complicating the diabetic foot ulceration when compared with other imaging modalities • Imaging in diabetic foot ulceration: a blinded comparison of infrared imaging with a plain film radiology, MRI, clinical assessment, and haematological and biochemical investigation- R.Harding, J.Jones, A. Griffiths, H. Morris – Royal Gwent & ST Woolos Hospital, Newport, Gwent, UK
The temperature on infrared imaging is significantly increased not only around the ulcer but also in the entire sole of the foot in patients with radiologically confirmed osteomyelitis. • Quantitative infrared imaging can point out the osteomyelitis installation, reducing morbidity and mortality by selecting those patients who will benefit from appropriate aggressive antibiotic therapy.
THERMOGRAPHY IN THE ASSESSMENT OF THE AMPUTATION LEVEL VIABILITY • Diabetic foot amputation: the need for an objective assessment tool (Wounds 15(7):241-245, 2003, Health management publication) • Thermography and later the clearance of the radioisotope were successfully used to determine the viability of skin flaps for below the knee amputation. The combination of these techniques yielded a success rate of 93% for transifibial amputation. ( Ninewells Hospital, Dundee, Scotland)
Amputation of the ischemic limb: selection of the optimum site by thermography – V.A.Spence, W.F.Walker, I.M.Troup – Vascular Laboratory, Ninewelles Hospital and Medical School , Dundee , Scotland • Results from 104 patients demonstrate that the thermographic method is a reliable indicator for the level of a major limb amputation.
IR lacks information about the local anatomy and only indirectly estimate the changes in the cutaneous microcirculatory blood supply. • The obtained data by merging both imaging techniques (IR&MRI) allows the determination of the extent of anatomic and physiological compromise, thus leading to a better and more adequate surgical intervention
MICROANGIOPATHY AND NEUROPATHY • These two topics can be discussed together, since the microangiopathy of the vasa nervorum contributes to the neuropathy pathogenesis, which in turn induces changes in the capillary circulation, thus partially compensating for the reduction in flow caused by the microangiopathy. • In the initial stages of neuropathy, when the microangiopathic changes are dominant, there is a symmetric hypothermia in the toes and the distal one third of the foot. Severe hypothermia may appear as “thermic amputation” , generated by a combination of obstructive microangiopathy and sympathetic hyperactivity caused by partial nerve damage.
After the onset of the neuropathic process, the skin temperature increases The diabetic neuropathy affects the microcirculation by increasing the blood flow through arteriovenous shunts, which are normally under the control of sympathetic system.
E.Boyko (Skin temperature in the neuropathic diabetic foot -2001) quotes a study in which the mean skin temperature on the plantar foot is between 33,2 and 33,5C among diabetic subjects with either painful or sensory neuropathy compared to a mean of 27,8 in diabetic subject without neuropathy.
The dynamic measurements of the plantar mean temperature can be useful in detecting the perfusion anomalies due to neuropathy . • The plantar temperature modifications are the result of the circulatory insufficiency, neuropath disorders, skeleton modifications, infections or any combinations of these factors.