Download
1 / 107
1.07k likes | 1.08k Views
This module covers changes in the Advocate Condell EMS System CE program, cardiac conduction system, 12-lead EKG interpretation, MI patterns, complications, interventions, and guidelines for acute coronary syndrome.

E N D
Overview of Revised CMC EMS System CE;12 Lead EKG’s February 2009 CE Site Code #107200E1209 Prepared by: Bill Glade, DC Wauconda Fire Department Sharon Hopkins, RN, BSN
Objectives • Upon successful completion of this module, the EMS provider will be able to accomplish the following: • Identify changes in the Advocate Condell EMS System CE program as taught in class. • Identify the appropriate components of the cardiac conduction system with the correct wave form on a rhythm strip. • Identify when it is appropriate to obtain an EKG • Identify the criteria for significant ST elevation following guidelines reviewed in class. • Identify EKG leads that view the anterior, inferior, lateral walls, and septum
Objectives • Recognize the patterns of an MI after viewing the components of a 12 lead EKG • Identify typical and atypical presentations of AMI • Identify complications associated with an inferior wall MI • Identify complications associated with an anterior/septal wall MI • Identify complications associated with a lateral wall MI • Identify interventions for complications related to heart block, pulmonary edema, and cardiogenic shock • Identify the SOP guidelines for the patient presenting with acute coronary syndrome aswritten in the Region X SOP’s
Objectives • State dosing and precautions for Aspirin, Nitroglycerin, and Morphine • Identify ED staff expectations of EMS personnel when calling the hospital to report a patient with ST elevation identified on a 12 lead EKG • Identify EMS expectations when delivering a patient to a hospital after ST elevation has been identified on a 12 lead EKG • Actively participate in 12 lead EKG scenario practice and discussion • Given a picture, correctly trace the order of the cardiac conduction system. • Given a manikin, correctly place electrodes to obtain a 12 lead EKG.
CMC EMS CE Process For 2009 • Educational committee formed to develop a new CE process that will be evolving • 7 CE’s presented by EMS staff • 2 CE’s presented by department members • Total of 27 hours of CE per year • Objectives and references for each CE sent to departments for preview • Each department will receive a detailed copy of the CE material for reference • CE power points will continue to be posted on the Condell website
2009 CE Process • All CE’s must be completed by year’s end • Medical Officer will oversee the completion for those not completing during EMS staff presentation • There will no longer be biannual exams • Quizzes will be administered at the completion of each CE • Successful completion is at 80% • Number of quiz questions may be variable dependent on topic and will be based on objectives • Handouts at class will only be material applicable to complete that topic and no longer the full power points
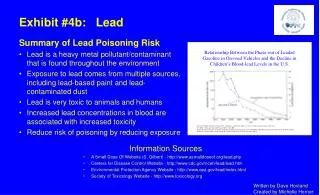
Why Are We doing Pre-hospital EKG’s? • Early recognition and fast, appropriate treatment can prevent the extension of an MI • Early recognition = early intervention • An important diagnostic tool will also be the patient’s general appearance
Cardiac Conduction System • Electrical cells arranged in a systematic pathway • Predominant pacemaker starting the electrical flow comes from the SA node • Electrical cells are part of the conduction system • Muscle cells are the mechanical cells
Cardiac Conduction System Purkinje fibers
EKG Waveforms • P wave represents atrial stimulation • P wave is rounded and upright • PR interval • Includes the P wave and the isoelectric PR segment • PR interval is the time it takes for an impulse to travel from the SA node through the internodal pathways toward the ventricles • Includes delay time in the AV node • Normal PR interval is 0.12 – 0.20 seconds
PR Interval Abnormalities • PR interval <0.12 seconds • Impulse did not begin in the normal pacemaker site of the SA node but somewhere in the atria • PR interval >0.20 seconds • There was a longer than normal delay transmitting the impulse through the AV node • A change in the PR interval measurement generally will not make the patient symptomatic
EKG Wave Forms cont’d • QRS complex • Consists of the Q, R, and S waves collectively • Represents ventricular depolarization or discharge of electrical energy throughout ventricular muscle • Larger than the P wave because ventricular depolarization involves a larger muscle mass than atrial depolarization • Palpation of a pulse is generated by ventricular depolarization (seen as the QRS complex) • Normal timing usually considered between 0.06 and 0.11 seconds • Normal is less than 0.12 seconds
QRS Complex Measurement • From beginning of Q wave – usually fairly straight forward • Stop measurement at end of S wave; not necessarily where QRS intersects baseline • On S wave, watch for small notch or other indicator that electrical flow is changing • Not always so easy to determine stop point • Do not include ST segment or T wave • Abnormally wide QRS indicates delay in conduction time through the ventricles
EKG Wave Forms cont’d • T wave • Represents ventricular repolarization • Repolarization is the phase of electrical activity where electrical charges (influenced primarily by sodium (Na+) and potassium (K+)) return to their original state and prepare to respond to the next electrical charge received • Atria repolarize during ventricular depolarization so the small atrial T wave is hidden during the larger QRS complex
When To Obtain a 12-Lead EKG • Any patient presenting with signs and/or symptoms of an acute coronary syndrome • Consider atypical AMI presentations • Elderly • Women • Patient with long standing history of diabetes • Any patient presenting with a Second degree Type II (classical) or 3rd degree heart block • Consider the origin from an AMI until proven otherwise
What Are We Looking For? • Abnormalities that indicate interruption in the blood flow to the myocardium • Plaque formation diminishes blood flow through the coronary arteries • Patients may be asymptomatic while damage silently develops • Plaque rupture begins a cascade of events that further compromises blood flow through the injured vessel(s) • This cascade of events could lead to an acute coronary syndrome (ie: acute MI)
Coronary Circulation • Coronary arteries and veins • Myocardium extracts the largest amount of oxygen as blood moves into general circulation • Oxygen uptake by the myocardium can only improve by increasing blood flow through the coronary arteries • If the coronary arteries are blocked, they must be reopened if circulation is going to be restored to that area of tissue supplied
12-Lead Electrodes • A lead is a tracing of the electrical activity between 2 electrodes • Leads view the heart from the front of the body • Top, bottom, right, and left side of heart • Leads view the heart as if it were sliced in half horizontally • Front, back, right, and left sides of heart • Each lead has a positive and a negative electrode
Standard 12-Lead EKG • Six limb leads • Leads I, II, III, aVR, aVL, aVF • Six chest leads (precordial leads) • V1, V2, V3, V4, V5, V6 • Information from 12 leads obtained from the attachment of only 10 electrodes
View The Leads Provide • II, III, aVF – view inferior wall of heart • V1 and V2 – view septal wall of heart • V3 and V4 – view anterior wall of heart • I, aVL, V5, V6 – view lateral wall of heart
Preparation for 12 Lead EKG • Skin preparation • Hair removal • clip hair if necessary so electrodes adhere • Clean and dry skin surface • gently rub skin area with gauze pad • need to remove skin oils & dead skin • if diaphoretic patient wipe with towel/gauze or use antiperspirant spray
Patient positioning • Preferably flat • Heart rotates position as the patient position changes • If patient is elevated, note that information on the EKG
Precordial Chest Leads For every person, each precordial lead placed in the same relative position • V1 - 4th intercostal space, R of sternum • V2 - 4th intercostal space, L of sternum • V4 - 5th intercostal space, midclavicular • V3 - between V2 and V4, on 5th rib • V5 - 5th intercostal space, anterior axillary line • V6 - 5th intercostal space, mid-axillary line
Precordial Leads 1st ICS 2nd ICS 3rd ICS
12 Lead EKG Printout • Standard format 81/2 x 11 paper • 12 lead format: I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Machines can analyze data obtained but humans must interpret data
Myocardial Insult • Ischemia • lack of oxygenation • ST depression or T wave inversion • permanent damage avoidable • Injury • prolonged ischemia • ST elevation • permanent damage avoidable • Infarct • death of myocardial tissue; damage permanent; may have Q wave
Why A Pre-hospital EKG? • EMS looking for ST segment elevation • Indicates injury that can be reversible if found early and acted upon early • TIME IS MUSCLE • The earlier the discovery of an acute cardiac event, the quicker the patient can receive the most appropriate care • EKG’s sent to the ED before patient arrival allows for the right personnel to be available to properly care for the patientin the most time efficient manner
What Do You Have to Do? • Obtain a 12 lead EKG • Evaluate the leads yourself as you are sending the 12 lead to the ED • Identify for the presence or absence of ST elevation • Report what you see, not just what is printed on the machine copy of the EKG • Upon arrival, hand a copy of your 12 lead to the ED staff while you give bedside report
Evaluating for ST Segment Elevation • Locate the J-point • Identify/estimate where the isoelectric line is noted to be • Compare the level of the ST segment to the isoelectric line • Elevation (or depression) is significant if more than 1 mm (one small box) is seen in 2 or more leads facing the same anatomical area of the heart (ie: contiguous leads)
The J Point • J point – where the QRS complex and ST segment meet • ST segment elevation - evaluated 0.04 seconds (one small box) after J point
Coved shape usually indicates acute injury • Concave shape is usually benign especially if patient is asympto-matic
Significant ST Elevation • ST segment elevation measurement • starts 0.04 seconds after J point • ST elevation • > 1mm (1 small box) in 2 or more contiguous chest leads (V1-V6) • >1mm (1 small box) in 2 or more anatomically contiguous leads • Contiguous lead • limb leads that “look” at the same area of the heart or are numerically consecutive chest leads
Contiguous Leads • Lateral wall: I, aVL, V5, V6 • Inferior wall: II, III, avF • Septum: V1 and V2 • Anterior wall: V3 and V4 • Posterior wall: V7-V9 (leads placed on the patient’s back 5th intercostal space creating a 15 lead EKG)
Evolution of AMI A - pre-infarct (normal) B - Tall T wave (first few minutes of infarct) C - Tall T wave and ST elevation (injury) D - Elevated ST (injury), inverted T wave (ischemia), Q wave (tissue death) E - Inverted T wave (ischemia), Q wave (tissue death) F - Q wave (permanent marking)
EKG monitoring • Evaluates electrical activity of the heart • Can indicate myocardial insult and location • ischemia - initial insult; ST depression seen • injury - prolonged myocardial hypoxia or ischemia; ST elevation seen • infarction - tissue death • dead tissue no longer contracts • amount of dead tissue directly relates to degree of muscle impairment • may show Q waves
Contiguous ECG Leads • EKG changes are significant when they are seen in at least two contiguous leads • Two leads are contiguous if they look at the same area of the heart or they are numerically consecutive chest leads
Groups of EKG Leads • Inferior wall - II, III, aVF • Septal wall - V1, V2 • Anterior wall - V3, V4 • Lateral wall - I, aVL, V5, V6 • aVR is not evaluated in typical groups • Standard lead placement does not look at posterior wall or right ventricle of the heart - need special lead placement for these views