Download

1 / 14
140 likes | 368 Views
Overview of MASH . MASH training . What is a MASH? . Multi Agency Safeguarding Hub A MASH is a centre which brings together agencies (and their information) in order to: identify risks to children at the earliest possible point and respond with the most effective interventions.

E N D
Overview of MASH MASH training
What is a MASH? • Multi Agency Safeguarding Hub • A MASH is a centre which brings together agencies (and their information) in order to: • identify risks to children at the earliest possible point • and respond with the most effective interventions. • A MASH carries out joint confidential screening, research and referral of vulnerable children. • Agencies work together to ensure vulnerable children are identified and properly cared for and protected
Why MASH? • The Children Act 2004 states that partners agencies must make arrangements to promote co-operation between relevant partner agencies to improve the well-being of children in their area • The inability of statutory safeguarding agencies to join up the information picture has been subject to persistent criticism and recommendation • MASH is a direct response to a number of serious case reviews including the Laming report which directly attributed the lack of good information sharing and communication to the subsequent death of a child • The Munro review highlights the value of co-located multi-agency teams dealing with referrals and decision making. MASH is singled out as good practice, with early evaluation showing improved decision making and outcomes for children
Safeguarding best practice • London wide police research proved that: • Early identification of children's needs provides the best outcomes for children • Early identification of risk has the best impact as its allows agencies to respond quickly with the most effective interventions
Essential criteria for a MASH • There are five core elements that must be included in a MASH • All notifications relating to safeguarding and promoting the welfare of children must go through the hub • Co-location of professionals from core agencies • The hub is fire walled, keeping MASH activity confidential and separate from operational activity • An agreed process for analysing and assessing risk, based on the fullest information picture and dissemination of a suitable information product to the most appropriate agency for necessary action • A process to identify victims and emerging harm through research and analysis
Partners in MASH • To be a MASH, it is a requirement that, as a minimum, the following partners are co-located: • Children’s social care • Police • Health • Education • Probation • Housing • Youth Offending Service • Redbridge MASH is represented by all the services listed above
Redbridge MASH • Redbridge MASH is located on the 3rd floor of Lynton House in Children's services • Staff are co-located in a secure area with limited access from the rest of Children’s services • The Head of the MASH has day to day management responsibility for the MASH. However, line management arrangements have not changed for partner agencies • Each agency will continue to access their own systems in the MASH. There is no requirement to access or learn new systems
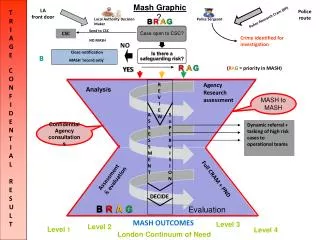
MASH process MERLIN Multi-agency referral Self referral Anonymous referral Other local authority referral Step 1 Open social care case: details sent to case worker Check protocol ICS Step 2 Check eCAF New case created on protocol Step 3 MASH MASH MASH Step 4 RAG rate & pass to social worker Initial screening on whether to MASH 4 hour target 1 day 1 day Step 5 Review and summary of collated information l Step 6 Decision making EI&FS CAF CPAT Advice and info Single agency response NFA
Redbridge MASH process • Step 1: Referral received into MASH screening • Step 2a/b: check Protocol to see whether the child/ family known to Redbridge children’s services. • Step 3: if no open case , create new case record and record any relevant information held on protocol ICS/eCaf. • Step 4a: Head of MASH decides whether to ‘MASH’ • Step 4b: Head of MASH RAG rates case
Redbridge MASH process (contd.) • Step 5: MASH case assigned to a social worker with agreed target timescale. • High Risk – RED: completed within 4 hours • Medium risk – AMBER: completed within 24 hours • Low risk – GREEN: completed within 24 hours • The social worker handling the case then asks colleagues in the multi-agency teams in the MASH to check the child/family details against their databases and to collate any information they may have about the child referred. • The information is collated within the timescales set through the RAG rating and returned to the social worker. • Social worker reviews and analyses information received from partner agencies within the MASH and summarises that information on a MASH record on protocol ICS. • Based on this information reviewed, the social worker recommends what further action should be taken.
Redbridge MASH process (contd.) • Step 6: The Head of the MASH or MASH Practice Manager reviews the MASH record and decides the most appropriate action to take in relation to that contact. • Pathways include: • CPAT • EI&FS • CAF • Information & Advice • Single Agency response • The Referral & Initial Screening Officer contacts the referrer to advise them as to what has happened with the referral.
Redbridge MASH criteria • All NSPCC/ anonymous referrals • All children whose identity is unknown • Children/ YP who may have been trafficked • Children/ YP at risk of sexual or other exploitation • Transient families • All referrals where DV is an issue (where there are children in the family under 5 years old or unborn) and additional information is needed to determine the threshold • All referrals where there has been a previous MARAC discussion • Referrals about a child found begging whereby additional information is needed to determine the threshold • Minor concerns about a child on a repeat basis • Children involved in gangs • All other referrals deemed appropriate by MASH manager
Expected outcomes of MASH • Streamlines the referral process • Improves communications between professionals • Child’s needs responded to quickly and effectively • Earlier identification of vulnerable children • Most appropriate professional delivers interventions to meet the needs identified • Reduction in number of professionals involved and avoids unnecessary duplication and visits