Download
1 / 1
10 likes | 132 Views
A Case of Palytoxin Poisoning of a Home Aquarium Enthusiast and His Family Christine Goss DO, David Levy DO Good Samaritan Hospital Medical Center, West Islip, NY Emergency Medicine Residency Program.

E N D
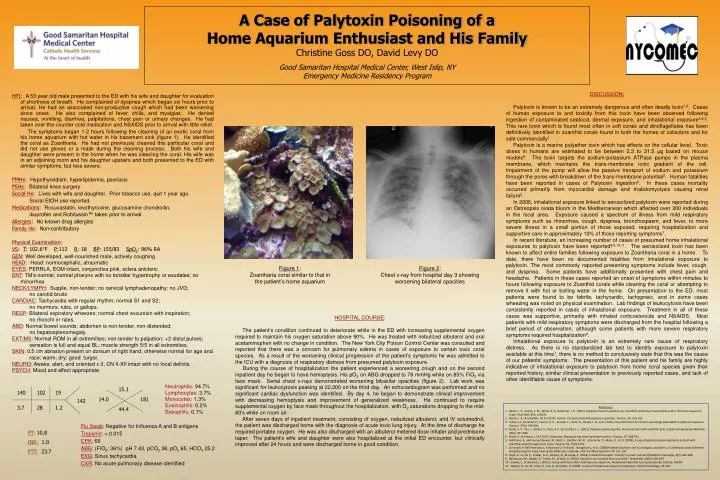
A Case of Palytoxin Poisoning of a Home Aquarium Enthusiast and His FamilyChristine Goss DO, David Levy DO Good Samaritan Hospital Medical Center, West Islip, NY Emergency Medicine Residency Program HPI: A 53 year old male presented to the ED with his wife and daughter for evaluation of shortness of breath. He complained of dyspnea which began six hours prior to arrival. He had an associated non-productive cough which had been worsening since onset. He also complained of fever, chills, and myalgias. He denied nausea, vomiting, diarrhea, palpitations, chest pain or urinary changes. He had taken over-the-counter cold medication and NSAIDS prior to arrival with little relief. The symptoms began 1-2 hours following the cleaning of an exotic coral from his home aquarium with hot water in his basement sink (figure 1). He identified the coral as Zoantharia. He had not previously cleaned this particular coral and did not use gloves or a mask during the cleaning process. Both his wife and daughter were present in the home whenhe was cleaning the coral. His wife was in an adjoining room and his daughter upstairs and both presented to the ED with similar symptoms, but less severe. PMHx: Hypothyroidism, hyperlipidemia, psoriasis PSHx: Bilateral knee surgery SocialHx:Lives with wife and daughter. Prior tobacco use, quit 1 year ago. Social EtOH use reported. Medications: Rosuvastatin, levothyroxine, glucosamine chondroitin. ibuprofen and Robitussin™ taken prior to arrival. Allergies: No known drug allergies Family Hx: Non-contributory Physical Examination: VS: T: 102.6°F P:112 R: 18 BP: 155/83 SpO2: 96% RA GEN: Well developed, well-nourished male, actively coughing HEAD: Head: normocephalic, atraumatic EYES: PERRLA, EOM intact, conjunctiva pink, sclera anicteric ENT: TM’s normal; normal pharynx with no tonsillar hypertrophy or exudates; no rhinorrhea NECK/LYMPH: Supple, non-tender; no cervical lymphadenopathy; no JVD; no carotid bruits CARDIAC: Tachycardia with regular rhythm; normal S1 and S2; no murmurs, rubs, or gallops. RESP: Bilateral expiratory wheezes; normal chest excursion with inspiration; no rhonchi or rales. ABD: Normal bowel sounds; abdomen is non-tender, non-distended; no hepatosplenomegaly. EXT/MS: Normal ROM in all extremities; non-tender to palpation; +2 distal pulses; sensation is full and equal BL; muscle strength 5/5 in all extremities. SKIN: 0.5 cm abrasion present on dorsum of right hand; otherwise normal for age and race; warm; dry; good turgor. NEURO: Awake, alert, and oriented x 3, CN II-XII intact with no focal deficits. PSYCH: Mood and affect appropriate. DISCUSSION: Palytoxin is known to be an extremely dangerous and often deadly toxin1,2. Cases of human exposure to and toxicity from this toxin have been observed following ingestion of contaminated seafood, dermal exposure, and inhalational exposure3,4,5. This rare toxin which is found most often in soft corals and dinoflagellates has been definitively identified in zoanthid corals found in both the homes of collectors and for sale commercially1. Palytoxin is a marine polyether toxin which has effects on the cellular level. Toxic doses in humans are estimated to be between 2.3 to 31.5 μg based on mouse models6. The toxin targets the sodium-potassium ATPase pumps in the plasma membrane, which maintains the trans-membrane ionic gradient of the cell. Impairment of the pump will allow the passive transport of sodium and potassium through the pores with breakdown of the trans-membrane potential2. Human fatalities have been reported in cases of Palytoxin ingestion6. In these cases mortality occurred primarily from myocardial damage and rhabdomyolysis causing renal failure2. In 2006, inhalational exposure linked to aerosolized palytoxin were reported during an Ostreopsis ovata bloom in the Mediterranean which affected over 200 individuals in the local area. Exposure caused a spectrum of illness from mild respiratory symptoms such as rhinorrhea, cough, dyspnea, bronchospasm, and fever, to more severe illness in a small portion of those exposed, requiring hospitalization and supportive care in approximately 10% of those reporting symptoms7. In recent literature, an increasing number of cases of presumed home inhalational exposures to palytoxin have been reported8,9,10,11. The aerosolized toxin has been known to affect entire families following exposure to Zoantharia coral in a home. To date, there have been no documented fatalities from inhalational exposure to palytoxin. The most commonly reported presenting symptoms include fever, cough, and dyspnea. Some patients have additionally presented with chest pain and headache. Patients in these cases reported an onset of symptoms within minutes to hours following exposure to Zoanthid corals while cleaning the coral or attempting to remove it with hot or boiling water in the home. On presentation to the ED, most patients were found to be febrile, tachycardic, tachypneic, and in some cases wheezing was noted on physical examination. Lab findings of leukocytosis have been consistently reported in cases of inhalational exposure. Treatment in all of these cases was supportive, primarily with inhaled corticosteroids and NSAIDS. Most patients with mild respiratory symptoms were discharged from the hospital following a brief period of observation, although some patients with more severe respiratory symptoms required hospitalization9. Inhalational exposure to palytoxin is an extremely rare cause of respiratory distress. As there is no standardized lab test to identify exposure to palytoxin available at this time1, there is no method to conclusively state that this was the cause of our patients’ symptoms. The presentation of this patient and his family are highly indicative of inhalational exposure to palytoxin from home coral species given their reported history, similar clinical presentation to previously reported cases, and lack of other identifiable cause of symptoms. Figure 1: Zoantharia coral similar to that in the patient’s home aquarium Figure 2: Chest x-ray from hospital day 3 showing worsening bilateral opacities 15.1 140 102 19 14.0 181 142 HOSPITAL COURSE: The patient’s condition continued to deteriorate while in the ED with increasing supplemental oxygen required to maintain his oxygen saturation above 90%. He was treated with nebulized albuterol and oral acetaminophen with no change in condition. The New York City Poison Control Center was consulted and reported that there was a concern for pulmonary edema in cases of exposure to certain toxic coral species. As a result of the worsening clinical progression of the patient’s symptoms he was admitted to the ICU with a diagnosis of respiratory distress from presumed palytoxin exposure. During the course of hospitalization the patient experienced a worsening cough and on the second inpatient day he began to have hemoptysis. His pO2 on ABG dropped to 76 mmHg while on 85% FiO2 via face mask. Serial chest x-rays demonstrated worsening bibasilar opacities (figure 2). Lab work was significant for leukocytosis peaking at 22,000 on the third day. An echocardiogram was performed and no significant cardiac dysfunction was identified. By day 4, he began to demonstrate clinical improvement with decreasing hemoptysis and improvement of generalized weakness. He continued to require supplemental oxygen by face mask throughout the hospitalization, with O2 saturations dropping to the mid-80’s while on room air. After seven days of inpatient treatment, consisting of oxygen, nebulized albuterol, and IV solumedrol, the patient was discharged home with the diagnosis of acute toxic lung injury. At the time of discharge he required portable oxygen. He was also discharged with an albuterol metered dose inhaler and prednisone taper. The patient’s wife and daughter were also hospitalized at the initial ED encounter, but clinically improved after 24 hours and were discharged home in good condition. 3.7 28 1.2 44.4 Neutrophils:94.7%Lymphocytes: 3.7%Monocytes: 1.3% Eosinophils: 0.2%Basophils: 0.1% References 1. Deeds, J. R., Handy, S. M., White, K. D., & Reimer, J. D. (2011). Palytoxin found in palythoa sp. zoanthids (anthozoa, hexacorallia) sold in the home aquarium trade. PLoS ONE, 6(4), e18235. 2. Deeds, J. R., & Schwartz, M. D. (2010). Human risk assocaited with palytoxin exposure. Toxicon, 56, 150-162. 3. Tubaro, A., Durando, P., Facero, G. D., Ansaldi, F., Icardi, G., Deeds, J. R., et al. (2011). Case definitions for human poisonings postulated to palytoxin exposure. Toxicon, 57(3), 478-495. 4. Nordt, S. P., Wu, J., Zahller, S., Clark, R. F., & Cantrell, F. L. (2011). Palytoxin poisoning after dermal contact with zoanthid coral. Journal of Emergency Medicine, 40(4), 397-399. 6. Riobo, P., & Franco, J. M. (2011). Palytoxins: Biological and chemical determination. Toxicon, 57, 368-375. 5. Hoffmann, K., Hermanns-Clausen, M., Buhl, C., Buchler, M. W., Schemmer, P., Mebs, D., et al. (2008). A case of palytoxin poisoning due to contact with zoanthid corals through a skin injury. Toxicon, 51, 1535-1537. 7. Ciminiello P, Dell’Aversano C, Fatturosso E, Forino M, Tartaglione L, et al. (2008) Putative palytoxin and its analogue, ovatoxin-a, in Ostreopsis ovata collected along the Ligurian coasts during the 2006 toxic outbreak. J Am Soc Mass Spectrom 19: 111-120 8. Payal, S., Su, M. K., Greller, H. A., Majlesi, N., & Gupta, A. (2013). Inhaled coral vapor: Toxicity in a tank. Journal Of Medical Toxicology, 9(3), 282-286. 9. Benrasconi, M., Berger, D., Tamm, M., & Stolz, D. (2012). Aquarism: An innocent leisure activity?. Respiration, 84(5), 436-439. 10. Snoeks, L., & Veenstra, J. (2012). Family with fever after cleaning a sea aquarium. Nederlandstijdschriftvoorgeneeskunde, 156(12), A4200. 11. Majlesi, N., Su, M., Chan, G., Lee, D., & Greller, H. (2008). A case of inhalational exposure to palytoxin. Clinical Toxicology, 46, 637. Flu Swab: Negative for Influenza A and B antigens Troponin: < 0.015 CPK: 66 ABG: (FIO2: 36%) pH 7.43, pCO2 38, pO2 65, HCO325.2 EKG: Sinus tachycardia CXR: No acute pulmonary disease identified PT: 10.8 INR:1.0 PTT:23.7