Download
1 / 1
10 likes | 160 Views
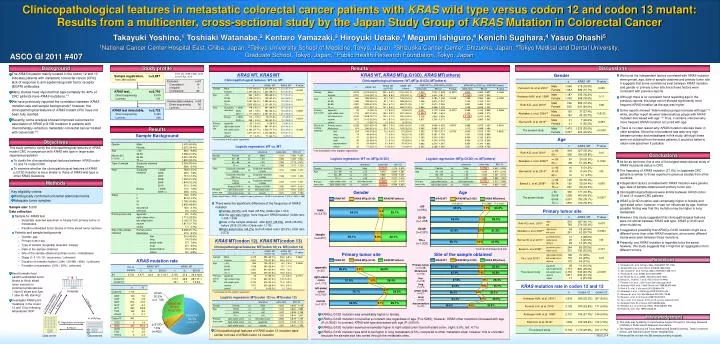
KRAS WT. KRAS WT. KRAS WT. KRAS WT. KRAS MT(p.G13D). KRAS MT(p.G13D). KRAS MT(p.G13D). KRAS MT(p.G13D). KRAS MT(others). KRAS MT(others). KRAS MT(others). KRAS MT(others). P=0.5285*. P=0.0002*. P=0.0001*. 69.5%. 7.5%. 23.0%. 6.4 %. 64.5%. 29.1%. 63.4%. 7.2%.

E N D
KRAS WT KRAS WT KRAS WT KRAS WT KRAS MT(p.G13D) KRAS MT(p.G13D) KRAS MT(p.G13D) KRAS MT(p.G13D) KRAS MT(others) KRAS MT(others) KRAS MT(others) KRAS MT(others) P=0.5285* P=0.0002* P=0.0001* 69.5% 7.5% 23.0% 6.4 % 64.5% 29.1% 63.4% 7.2% 29.3% 61.9% 6.7% 31.3% 59.1% 8.8% 32.1% 60.1% 8.0% 31.9% No. of sample KRASWT KRASMT n % 95%CI n % 95%CI n % All 5,732 3,577 62.4 61.1-63.7 2,155 37.6 36.3-38.9 Hospitals Codon12 1,714 Codon12 Codon13 1,714 441 29.9 7.7 28.7-31.1 7.0-8.4 AGT CGT GAT GCT GTT TGT others 120 15 814 107 493 162 3 7.0 0.9 47.5 6.2 28.8 9.5 0.1 2. Enrollment confirmation 1. Sample registration 3. Sample 6. Result Codon13 441 4.KRAS test CGC GAC GAG TGC others 6 420 1 11 3 1.4 95.2 0.2 2.5 0.7 2’. Registration information 5. Result Data center Laboratories Clinicopathological features in metastatic colorectal cancer patients with KRAS wild type versus codon 12 and codon 13 mutant: Results from a multicenter, cross-sectional study by the Japan Study Group of KRAS Mutation in Colorectal Cancer Takayuki Yoshino,1Toshiaki Watanabe,2Kentaro Yamazaki,3Hiroyuki Uetake,4Megumi Ishiguro,4Kenichi Sugihara,4Yasuo Ohashi5 1National Cancer Center Hospital East, Chiba, Japan,2Teikyo University School of Medicine, Tokyo, Japan, 3Shizuoka Cancer Center, Shizuoka,Japan, 4Tokyo Medical and Dental University, Graduate School, Tokyo, Japan, 5Public Health Research Foundation, Tokyo, Japan ASCO GI 2011 #407 Background Study profile Results Discussions The KRAS mutation mainly located in the codon 12 and 13 indicates patients with metastatic colorectal cancer (CRC) lack of response to anti-epidermal growth factor receptor (EGFR) antibodies. Many studies have reported that approximately 30-40% of CRC patients have KRASmutations.1-3 We have previously reported the correlation between KRAS mutation rate and sample backgrounds;4 however, the clinicopathological features of KRAS mutant CRC have not been fully clarified. Recently, some analysis showed improved outcomes for association of KRAS p.G13D mutation in patients with chemotherapy-refractory metastatic colorectal cancer treated with cetuximab.5-6 KRAS WT, KRAS MT KRAS WT, KRAS MT(p.G13D), KRAS MT(others) From Oct. 2009 to Mar. 2010 Cut-off: Apr. 2010 Gender Sample registration, n=5,887 from 389 facilities • We found the independent factors correlated with KRAS mutation were gender, age, date of sample obtained and primary tumor site. It suggests that some correlations exist between KRAS mutation and gender or primary tumor site since these factors were consistent with previous reports • Although there is no consistent trend regarding age in the previous reports, this large cohort showed significantly more frequent KRAS mutation as the age was higher. • Some reports showed “Adenomatous polyps increase with age”;15 while,another report showed “adenomatous polyps with KRAS mutation decreased with age”.16 Thus, it remains unknown why more frequent KRAS mutation occurred with age. • There is no clear reason why KRAS mutation rate was lower in older samples. Since the concordance rate was very high between primary and metastases in this study, although these were not obtained from the same patients, it would be better to obtain new specimen if possible. Clinicopathological features: WT vs. MT Clinicopathological features: WT, MT(p.G13D), MT(others) Excluded, n=97 Cancelation 14 Ineligible 1 Uncollected 82 KRAS test, n=5,790 Direct sequencing 5,479 Luminex 311 Undetectable samples, n=58 Direct sequencing 56 Luminex 2 KRAS test detectable, n=5,732 Direct sequencing 5,423 Luminex 309 Results Sample Background Age * not included in the logistic regression Objectives Logistic regression: WT vs. MT This study aimed to clarify the clinicopathological features of KRAS mutant CRC in comparison with KRAS wild type in large-scale Japanese population. * not included in the logistic regression Conclusions Logistic regression: WT vs. MT(p.G13D) Logistic regression: MT(p.G13D) vs. MT(others) • To clarify the clinicopathological features between KRAS codon 12 and 13 mutant CRC. • To examine whether the clinicopathological features of KRAS p.G13D mutation is more similar to those of KRAS wild type or other KRAS mutations. • As far as we know, this is one of the largest observational study of KRAS mutational status in CRC. • The frequency of KRAS mutation (37.6%) in Japanese CRC patients is similar to those reported in previous studies from other countries. • Independent factors correlated with KRAS mutation were gender, age, date of sample obtained and primary tumor site. • Clinicopathological features were similar between KRAS codon 12 and 13 mutant CRC patients. • KRAS p.G13D mutation was remarkably higher in female and right-sided colon; however, it was not influenced by age. Another possible finding was that this mutation may be higher in lung metastasis. • However, this study suggested that clinicopathological features were not similar between KRAS wild type, KRAS p.G13D and other mutations. • It suggests a possibility that KRAS p.G13D mutation might be a different tumor than other KRAS mutations, since some different trends were seen between those mutations. • Presently, any KRAS mutation is regarded to be the same; however, this study suggests that it might be an aggregation from different tumors. Methods • Key eligibility criteria • Histologically confirmed colorectal adenocarcinoma • Adequate tumor samples Gender Age [Odds ratio of biopsy (2009=<) against surgery specimen (<2006)is estimated as (1.003×1.482)=1.486] • There were the significant difference of the frequency of KRAS mutation • Female (40.9%) and male (35.5%) (Odds-ratio 1.210) • As the age was higher, more frequent KRAS mutation (Odds-ratio 1.308-1.399) • Date of the sample obtained: after 2007 (38.6%), 2006 (36.6%), before 2005 (33.6%) (Odds-ratio 1.118) • Right-sided colon (48.2%) and left-sided colon (29.3%) (Odd ratio 2.272) <50(n=560) Sample size: 5,000 Data collection: • Sample for KRAS test • Surgically resected specimen or biopsy from primary tumor or metastases • Paraffin-embedded tumor blocks or thinly sliced tumor sections • Patients and sample backgrounds • Gender, age • Primary tumor site • Type of sample (surgically resected / biopsy) • Date of the sample obtained • Site of the sample obtained (primary tumor / metastases) • Stage (l / ll / lll / IV / recurrence / unknown) • Duration of formalin fixation (<24h / 24-48h / 48h< / unknown) • Formalin concentration (10% / 20% / unknown) male (n=3,475) Primary tumor site 50-59 (n=1,258) 60-69 (n=2,081) female (n=2,257) KRAS MT(codon 12), KRAS MT(codon 13) 70=< (n=1,833) Clinicopathological features: MT(codon 12) vs. MT(codon 13) *Cochran-Armitage trend test Primary tumor site Site of the sample obtained References KRAS mutation rate 1. Karapetis CS. et al. N Engl J Med. 2008;359:1757-1765. 2. Amado RG. et al. J Clin Oncol. 2008;26:1626-1634. 3. Van Cutsem E. et al. N Engl J Med. 2009;360:1408-1417. 4. Yamazaki K. et al. ESMO 2010 Abst.595P 5. De Roock W. et al. JAMA. 2010;304:1812-1820. 6. Bando H., Yoshino T. et al. ASCO-GI 2011 #448 7. Ferreira C.G. et al. J Clin Oncol 2010;28,suppl:3614. 8. Andreyev HJN. et al. J Natl Cancer Inst 1998;90:675-684. 9. Roth A.D. et al. J clin oncol 2010;28:466-474. 10. Abubaker J. et al. J Pathology 2009;219:435-445. 11. Bennani B. et al. Int J Biol Markers 2010;25:179-84. 12. Barault L. et al. Int J Cancer 2008;122:2255-9. 13. Tie J. et al. Int J Cancer. 2010 Jul 15. [online ahead of print] 14. Andreyev HJN. Br J Cancer 2001;85:692-696. 15. Winawer S.J. et al. N Engl J Med. 1993;328:901-906. 16. Rashid A. et al. Gut. 1999;44:826-33. Primary tumor (n=5,258) 62.4% 30.3% 7.3% appendix (n=25) 36.0% 8.0% 56.0% Metastasis (n=474) 62.4% 30.2% 7.4% • Send formalin-fixed paraffin-embedded tumor blocks or thinly sliced tumor sections to commercial laboratories (10µm 5 slices and 3µm 1 slice for HE staining) • Investigate KRAS point mutations in the codon 12 and 13 by following laboratories’ SOP right-sided colon (n=1,713) liver (n=216) 67.6% 26.4% 6.0% 51.8% 9.9% 38.4% lung (n=74) KRAS mutation rate in codon 12 and 13 64.9% 25.7% 9.5% left-sided colon (n=2,160) 4.7 % lymph node (n=37) 70.7% 24.5% * not included in the logistic regression 59.5% 35.1% 5.4% others 30.3% (n=1,735) Logistic regression: MT(codon 12) vs. MT(codon 13) local (n=45) 64.4% 28.9% 6.7% rectum (n=1,817) 62.9% 8.1% 29.1% KRAS MT 37.6% (n=2,155) dissemination (n=70) 48.6% 42.9% 8.6% • KRAS p.G13D mutation was remarkably higher in female. • KRAS p.G13D mutation occurred at a constant rate regardless of age (P=0.5285); however, KRAS other mutations increased with age (P=0.0002). In contrast, KRAS wild type decreased with age (P=0.0001). • KRAS p.G13D mutation seemed remarkably higher in right-sided colon than left-sided colon. (right:9.9%, left:4.7%) • KRAS p.G13D mutation was tend to be higher in lung metastasis (9.5%) compared to other metastatic sites; however, this is uncertain because the sample size has varied through the metastatic sites. KRAS WT 62.4% (n=3,577) Acknowledgement • This study was funded by Comprehensive Support Project for Oncology Research (CSPOR) of Public Health Research Foundation. • The research institutes are Tokyo Medical and Dental University, Teikyo University School, and National Cancer Center Hospital East. • We would like to thank the 389 sample providing hospitals. p.G13D 7.3% (n=420) Clinicopathological features of KRAS codon 13 mutation were similar to those of KRAS codon 12 mutation * 755/2,214