Download
1 / 26
280 likes | 411 Views
Encephalitis Benedict Daniel Michael Benedict Michael (NIHR Doctoral Research Registrar in Neurology) works at the Institute of Infection ad Global Health, University of Liverpool and the Walton Centre for Neurology NHS Foundation Trust, Liverpool.

E N D
Encephalitis Benedict Daniel Michael Benedict Michael (NIHR Doctoral Research Registrar in Neurology) works at the Institute of Infection ad Global Health, University of Liverpool and the Walton Centre for Neurology NHS Foundation Trust, Liverpool. He has a particular interest in both clinical practice and research into neurological infectious diseases and the para-infectious neuroimmunological response. He is also involved in the development and dissemination of national guidelines for neurological diseases. Edited by Prof Tom Solomon and Dr Agam Jung • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment This session provides an overview of issues relating to the clinical features, acute investigation, diagnosis and management of encephalitis.
Learning Objectives • By the end of this session you will be able to: • State the pathogenesis of encephalitis • Describe the clinical features which should raise suspicion of encephalitis • Define the appropriate acute investigations which should be performed for patients with suspected encephalitis • Explain the appropriate treatment for encephalitis • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
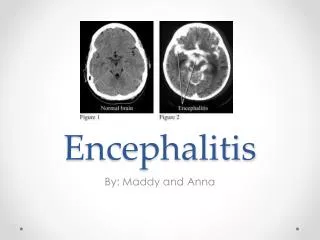
Overview This session explores the aetiology, clinical features, acute investigations and treatment of patients with suspected encephalitis. First it examines why cases of encephalitis are missed or diagnosed and treated late. This is important as mortality rates are 70% in untreated cases and can be as low as 10-20% if patients are treated early. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment Then it explains how pitfalls in missing or delaying diagnosis can be avoided. Finally, it provides a clear, structured approach to investigation, diagnosis and treatment of encephalitis. The first section begins with an overview of encephalitis. Image from: http//pathology.mc.duke.edu/neuropath/CNSlecture2/hsv.jp
Pathogenesis of encephalitis I • Encephalitis is defined as inflammation of the brain parenchyma. This is most commonly due to infection, typically with viruses, or less commonly, intracellular bacteria and mycobacteria. • The most common viral causes of encephalitis are: • Herpes simplex virus (HSV)1 • Varicella zoster virus (VZV) • These account for approximately 19% and 5% of cases respectively. • Other causes of encephalitis include an 'acute disseminated encephalomyelitis' (ADEM) in approximately 11%, where encephalitis follows infection or vaccination. Additionally, antibody-mediated causes for encephalitis have been identified, most commonly those due to anti-NMDA and anti-VGKC antibodies, which account for 4% and 3% of cases respectively. The former is often a paraneoplastic process. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Pathogenesis of encephalitis II The aetiology of encephalitis varies widely by age, geographical location and immune status. The table below demonstrates the findings of a recent Health Protection Agency study of 203 patients in the UK. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment ADEM= Acute disseminated encephalomyelitis; ANT= Antibody-associated cause; HSV= Herpes simplex virus; MTB= Mycobacterium tuberculosis; VZV=Varicella zoster virus
Unknown Aetiology In approximately 40% of cases, the aetiology remains unknown. Urgent and thorough investigation, particularly examination of the cerebrospinal fluid (CSF) by performing a lumbar puncture (LP), maximises the chance of identifying the cause. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment This figure is derived from a systematic review of studies of encephalitis by country demonstrating the proportion of cases in which a pathogen is not identified.
Causes of Encephalitis I Encephalitis can be caused by a wide range of pathogens in the immunocompetent and an even wider variety in the immunocompromised. Variation between the proportion of cases due to the common pathogens in the immunocompetent and the immunocompromised are outlined in a table on the following page from a recent study conducted in England. There is significant global variation in the incidence of causal pathogens reflecting endemic rates of human immunodeficiency virus (HIV) and tuberculosis infection, malnutrition and vaccination programmes. Additionally, viral vector prevalence is particularly important for arbovirus encephalitis, such as Japanese encephalitis virus and West Nile virus. Although this is typically limited to developing countries, recent outbreaks of the latter virus have been seen in the USA and southern Europe. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Causes of Encephalitis II • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Suspicious clinical features I The classical clinical features are headache or altered or reduced consciousness or personality or behaviour change in a patient with a fever or history of a febrile illness. However, as demonstrated in the table on the following page, approximately 28% of patients with encephalitis are not febrile on admission. Indeed, in the same study 11% of patients with proven HSV encephalitis were not febrile on admission. Additionally, encephalitis should be considered for patients with new onset seizures, particularly if refractory. Altered consciousness, personality or behaviour should not be attributed to an infection outside of the central nervous system, such as a urinary tract infection, in an otherwise healthy patient unless there is strong evidence for this. Indeed, many patients with proven encephalitis will have gastrointestinal, respiratory or urinary symptoms. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Suspicious clinical features II • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment Adapted from Granerod et al. 2010
Suspicious clinical features III The wide range of clinical features require that many patients are investigated. In a recent study, of 217 patients with suspected CNS infections at 10 hospitals, 44 had the diagnosis confirmed. Clinical features supporting the diagnosis of a CNS infection are outlined in the table below. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Suspicious clinical features IV • Often there is both clinical and histopathological overlap between encephalitis and meningitis and the term 'meningoencephalitis' is often used. • Nevertheless, clinical features reflecting involvement of the brain parenchyma may point towards a diagnosis of encephalitis: • Seizures • Focal neurological signs (including movement disorders) • Neuropsychiatric features • Do not rely on a low Glasgow coma score as this is a very crude proxy of cerebral dysfunction. Indeed, in the two recent studies described only 5 of 13 (38%) had a GCS<15 and 37 of 203 (18%) had a GCS <8. • Instead get a collateral history and assess this and the patient carefully for evidence of altered personality, behaviour and cognition, including neuro-psychiatric features. Never dismiss the statement of a friend or relative that a patient is 'not quite themselves'. • Perform a full neurological examination, • including mental state assessment and • fundoscopy. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Acute Diagnosis I A diagnostic algorithm can be found on the following page. CSF examination from a lumbar puncture (LP) is the most important investigation as this can confirm or refute the diagnosis and direct treatment towards a viral, bacterial or mycobacterial pathogen. Lumbar Puncture: An LP should be performed urgently for all patients in whom encephalitis is suspected unless there are clinical contraindications, as outlined on the following page. These clinical features have been found to be reliable and sensitive at identifying which patients are likely to have brain shift precluding an LP. CT scan: If the clinical contraindications are present, a computed tomography (CT) scan of the brain should be arranged urgently and if this does not show the outlined features, an urgent LP performed. Coagulation abnormalities Patients with coagulation abnormalities should these corrected before performing a LP and platelet count should be >100x109/L. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Acute Diagnosis II • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Investigations I Often clinicians inappropriately request a CT to 'rule out raised intracranial pressure before an LP'. However, a CT scan cannot do this and indeed an LP may be safe in patients with raised intracranial pressure. The CT should only be performed before an LP to identify if significant brain shift is present, thereby precluding an LP in those patients in whom it is likely, as determined by the clinical features outlined. Delays in performing the LP have been demonstrated to delay the diagnosis and treatment in acute CNS infections and this results in increased morbidity and mortality. The routine CSF parameters and interpretation are shown in the table on the following page. The first CSF white cell count may be normal in approximately 10% of cases. If the clinical suspicion remains, the LP should be repeated 24-48 hours later. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Investigations II • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
A staged approach to pathogen detection I Although a wide range of pathogens can cause encephalitis, a staged approach to pathogen identification as outlined in the table below provides a pragmatic way to proceed: • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
A staged approach to pathogen detection II The ancillary investigations outlined in the table opposite can establish concomitant systemic infection, but not necessarily the cause of the encephalitis. Samples from sterile sites, such as vesicle swabs for VZV are more likely to represent active infection than non-sterile sites, such as faeces for enteroviruses, as this may represent asymptomatic shedding. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
MRI and EEG • Additionally, euro-imaging, preferably magnetic resonance imaging (MRI), can identify evidence of brain parenchymal inflammation. This may also point towards the aetiology, for example: • Fronto-temporal changes may be seen in HSV encephalitis • Hippocampal changes in limbic encephalitis, such as that due to VGKC antibodies • Basal ganglia changes in some arboviralencephalitides • Brain stem changes are seen in rhombencephalitis, such as that due to Listeriamonocytogenes • Electroencephalography (EEG) should be requested when subtle-motor or non-convulsive status epilepticus is suspected, for example a patient with fluctuating levels of consciousness, or if subtle motor features such as eye lid movement, are present.EEG can also be useful if it is unclear if the presentation is due to a primary psychiatric cause or encephalitis. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Appropriate treatment for encephalitis • Attention should be given to: • Oxygenation • Fluid and hydration • Nasogastric or parenteral feeding • Treating the complications, such as pneumonia • Patients with a reduced coma score or impaired gag reflex, should be assessed by an intensive care team. • In most immunocompetent patients, aciclovir (10mg/kg three times/day) should be given intravenously as soon as there is a strong suspicion of viral encephalitis, based on the clinical presentation and initial CSF and/or imaging findings. If performing these investigations is likely to lead to long delays and the clinical suspicion is strong, then treatment should be started at once. • Aciclovir is a nucleoside analogue that reduces mortality from around 70% to 10-20% when encephalitis is due to herpes viruses including HSV and VZV. However, approximately 60% of survivors have significant neurological and neuro-psychiatric morbidity. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Renal Function Renal function should be monitored closely and adequate hydration maintained because of the rare risk of renal failure. Other rare adverse effects include local inflammation at the site of the intravenous cannula, hepatitis, and bone marrow failure. As it is often not possible to determine whether the infection is due to a virus or bacteria in the acute phase, it is reasonable to commence both aciclovir and a 3rd generation cephalosporin. Nevertheless, due to the risks of opportunistic infection, antibiotic resistance and nephrotoxicity, the prescription of antimicrobials should be regularly reviewed in the light of test results. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Treatments in use Antibody-mediated encephalitis, such as that due to voltage-gated potassium channel or N-methyl D-apartate receptor antibodies, often respond well to immune suppression. This includes plasma exchange or intravenous steroids in the acute phase and prolonged immunesuppression, such as with cyclosporin, to maintain remission. However, there is currently no consensus clinical guidance as to which treatments to use. Therefore, these patients should be managed under specialist neurology supervision. Patients and their family should be put in contact with patient-orientated support services, such as the Encephalitis Society, so that they have improved access to information, neuropsychological and social support. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
2012 guidelines for the management of suspected viral encephalitis Click below to view a flow chart summary of the most recent guidelines on the management of encephalitis: For the full guidelines see: Journal of Infection 2012, 64; issue 4: 347–373 (adult) and issue 5: 449-477 (children). • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment Association of British Neurologists and British Infection Association guidelines 2012 on management of suspected viral encephalitis in adults and children
Key Points • Encephalitis is an important neurological emergency because early diagnosis and treatment decreases the risk of mortality and significant neurological morbidity. • There are a wide range of clinical features that can be seen, but the presence of acute alteration or reduction in consciousness, or personality or behaviour change should raise suspicion of encephalitis. • Not all patients will be febrile or have a history of fever. If clinical suspicion remains, two lumbar punctures, performed 24-48 hours apart are required to exclude the diagnosis. • The lumbar puncture does not have to be delayed for neuro-imaging unless specific clinical contraindications are present • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Summary • Having completed this session you will now be able to: • State the pathogenesis of encephalitis • Describe the clinical features which should raise suspicion of encephalitis • Define the appropriate acute investigations which should be performed for patients with suspected encephalitis • Explain the appropriate treatment for encephalitis • References and further reading: • Solomon T, Hart I, Beeching NJ. Viral Encephalitis: A clinician's guide. Practical Neurology 2007; 7:288-305. • Granerod J, Ambrose HE, Davies NWS, Clewley JP et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infectious Diseases 2010; 10: 835–44. • Michael BD, Sidhu M, Stoeter D, Roberts M, et al. The Epidemiology and Management of Adult Suspected Central Nervous System Infections - a retrospective cohort study in the NHS Northwest Region. Quarterly Journal of Medicine 2010; doi:10.1093/qjmed/hcq121. • Granerod J, Tam CC, Crowcroft NS, et al. Challenge of the unknown : A systematic review of acute encephalitis in non-outbreak situations. Neurology 2010;75;924. • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment
Question 1 • Encephalitis • Learning Objectives • Overview • Pathogenesis • Cases of unknown aetiology • Causes • Suspicious clinical features • Acute diagnosis • Investigations • Staged approach to pathogen detection • MRI & EEG • Key management • Renal Function • Other treatments • 2012 Guidelines • Key Points • Summary • Self assessment Which one of the below statements is correct? All patients with encephalitis have a fever on admission or a history of fever. The Glasgow Coma Scale (GCS) is a sensitive marker of brain dysfunction. A computed tomography (CT) scan cannot exclude raised Intracranial Pressure (ICP). Raised ICP is a contraindication to Lumbar Puncture. If the initial LP shows a normal white cell count and clinical suspicion remains the LP should be repeated 6 days later.