Download
1 / 1
10 likes | 65 Views
Influenza Virus: A Significant Etiology in Adult Patients Hospitalized with Lower Respiratory Tract Infections in Jefferson County, Kentucky

E N D
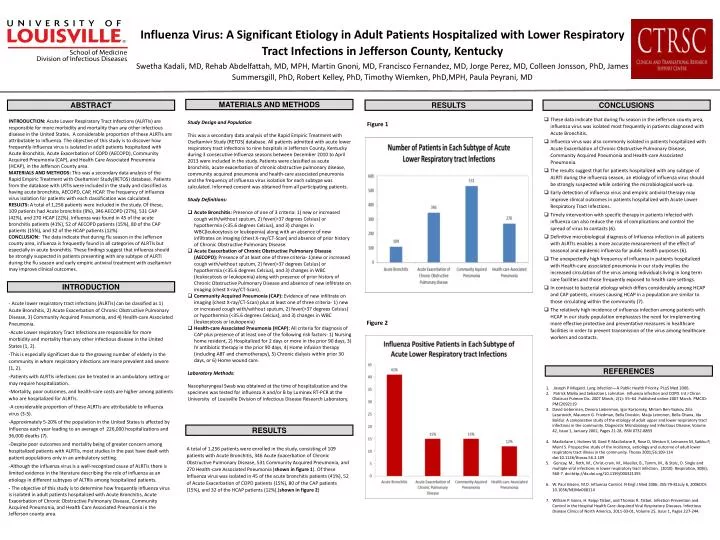
Influenza Virus: A Significant Etiology in Adult Patients Hospitalized with Lower Respiratory Tract Infections in Jefferson County, Kentucky SwethaKadali, MD, Rehab Abdelfattah, MD, MPH, Martin Gnoni, MD, Francisco Fernandez, MD, Jorge Perez, MD, Colleen Jonsson, PhD, James Summersgill, PhD, Robert Kelley, PhD, Timothy Wiemken, PhD,MPH, Paula Peyrani, MD MATERIALS AND METHODS ABSTRACT RESULTS CONCLUSIONS • These data indicate that during flu season in the Jefferson county area, influenza virus was isolated most frequently in patients diagnosed with Acute Bronchitis. • Influenza virus was also commonly isolated in patients hospitalized with Acute Exacerbation of Chronic Obstructive Pulmonary Disease, Community Acquired Pneumonia and Health-care Associated Pneumonia. • The results suggest that for patients hospitalized with any subtype of ALRTI during the influenza season, an etiology of influenza virus should be strongly suspected while ordering the microbiological work-up. • Early detection of influenza virus and empiric antiviral therapy may improve clinical outcomes in patients hospitalized with Acute Lower Respiratory Tract Infections. • Timely intervention with specific therapy in patients infected with influenza can also reduce the risk of complications and control the spread of virus to contacts (6). • Definitive microbiological diagnosis of Influenza infection in all patients with ALRTIs enables a more accurate measurement of the effect of seasonal and epidemic influenza for public health purposes (6). • The unexpectedly high frequency of influenza in patients hospitalized with Health-care associated pneumonia in our study implies the increased circulation of the virus among individuals living in long term care facilities and those frequently exposed to health care settings. • In contrast to bacterial etiology which differs considerably among HCAP and CAP patients, viruses causing HCAP in a population are similar to those circulating within the community (7). • The relatively high incidence of influenza infection among patients with HCAP in our study population emphasizes the need for implementing more effective protective and preventative measures in healthcare facilities in order to prevent transmission of the virus among healthcare workers and contacts. INTRODUCTION: Acute Lower Respiratory Tract Infections (ALRTIs) are responsible for more morbidity and mortality than any other infectious disease in the United States. A considerable proportion of these ALRTIs are attributable to influenza. The objective of this study is to discover how frequently Influenza virus is isolated in adult patients hospitalized with Acute Bronchitis, Acute Exacerbation of COPD (AECOPD), Community Acquired Pneumonia (CAP), and Health Care Associated Pneumonia (HCAP), in the Jefferson County area. MATERIALS AND METHODS: This was a secondary data analysis of the Rapid Empiric Treatment with Oseltamivir Study(RETOS) database. Patients from the database with LRTIs were included in the study and classified as having acute bronchitis, AECOPD, CAP, HCAP. The frequency of influenza virus isolation for patients with each classification was calculated. RESULTS: A total of 1,256 patients were included in the study. Of these, 109 patients had Acute bronchitis (9%), 346 AECOPD (27%), 531 CAP (42%), and 270 HCAP (22%). Influenza was found in 45 of the acute bronchitis patients (41%), 52 of AECOPD patients (15%), 80 of the CAP patients (15%), and 32 of the HCAP patients (12%). CONCLUSION: The data indicate that during flu season in the Jefferson county area, influenza is frequently found in all categories of ALRTIs but especially in acute bronchitis. These findings suggest that influenza should be strongly suspected in patients presenting with any subtype of ALRTI during the flu season and early empiric antiviral treatment with oseltamivir may improve clinical outcomes. • Study Design and Population • This was a secondary data analysis of the Rapid Empiric Treatment with Oseltamivir Study (RETOS) database. All patients admitted with acute lower respiratory tract infections to nine hospitals in Jefferson County, Kentucky during 3 consecutive Influenza seasons between December 2010 to April 2013 were included in the study. Patients were classified as acute bronchitis, acute exacerbation of chronic obstructive pulmonary disease, community acquired pneumonia and health-care associated pneumonia and the frequency of influenza virus isolation for each subtype was calculated. Informed consent was obtained from all participating patients. • Study Definitions: • Acute Bronchitis: Presence of one of 3 criteria: 1) new or increased cough with/without sputum, 2) fever(>37 degrees Celsius) or hypothermia (<35.6 degrees Celsius), and 3) changes in WBC(leukocytosis or leukopenia) along with an absence of new infiltrates on imaging (chest X-ray/CT-Scan) and absence of prior history of Chronic Obstructive Pulmonary Disease. • Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD):Presence of at least one of three criteria- 1)new or increased cough with/without sputum, 2) fever(>37 degrees Celsius) or hypothermia (<35.6 degrees Celsius), and 3) changes in WBC (leukocytosis or leukopenia) along with presence of prior history of Chronic Obstructive Pulmonary Disease and absence of new infiltrate on imaging (chest X-ray/CT-Scan). • Community Acquired Pneumonia (CAP):Evidence of new infiltrate on imaging (chest X-ray/CT-Scan) plus at least one of three criteria- 1) new or increased cough with/without sputum, 2) fever(>37 degrees Celsius) or hypothermia (<35.6 degrees Celcius), and 3) changes in WBC (leukocytosis or leukopenia) • Health-care Associated Pneumonia (HCAP):All criteria for diagnosis of CAP plus presence of at least one of the following risk factors- 1) Nursing home resident, 2) Hospitalized for 2 days or more in the prior 90 days, 3) IV antibiotic therapy in the prior 90 days, 4) Home infusion therapy (including ABT and chemotherapy), 5) Chronic dialysis within prior 30 days, or 6) Home wound care. • Laboratory Methods: • Nasopharyngeal Swab was obtained at the time of hospitalization and the specimen was tested for influenza A and/or B by Luminex RT-PCR at the University of Louisville Division of Infectious Disease Research Laboratory. Figure 1 INTRODUCTION - Acute lower respiratory tract infections (ALRTIs) can be classified as 1) Acute Bronchitis, 2) Acute Exacerbation of Chronic Obstructive Pulmonary Disease, 3) Community Acquired Pneumonia, and 4) Health-care Associated Pneumonia. -Acute Lower respiratory Tract Infections are responsible for more morbidity and mortality than any other infectious disease in the United States (1, 2). -This is especially significant due to the growing number of elderly in the community in whom respiratory infections are more prevalent and severe (1, 2). -Patients with ALRTIs infections can be treated in an ambulatory setting or may require hospitalization. -Mortality, poor outcomes, and health-care costs are higher among patients who are hospitalized for ALRTIs. -A considerable proportion of these ALRTIs are attributable to influenza virus (3-5). -Approximately 5-20% of the population in the United States is affected by Influenza each year leading to an average of 226,000 hospitalizations and 36,000 deaths (7). -Despite poor outcomes and mortality being of greater concern among hospitalized patients with ALRTIs, most studies in the past have dealt with patient populations only in an ambulatory setting. -Although the influenza virus is a well-recognized cause of ALRTIs there is limited evidence in the literature describing the role of influenza as an etiology in different subtypes of ALTRIs among hospitalized patients. -The objective of this study is to determine how frequently influenza virus is isolated in adult patients hospitalized with Acute Bronchitis, Acute Exacerbation of Chronic Obstructive Pulmonary Disease, Community Acquired Pneumonia, and Health Care Associated Pneumonia in the Jefferson county area. Figure 2 REFERENCES Joseph P Mizgerd. Lung Infection—A Public Health Priority. PLoS Med 2006. Patrick Mallia and Sebastian L Johnston. Influenza infection and COPD. Int J Chron Obstruct Pulmon Dis. 2007 March; 2(1): 55–64. Published online 2007 March. PMCID: PMC2692119 David Lieberman, Devora Lieberman, Igor Korsonsky, Miriam Ben-Yaakov, ZiliaLazarovich, Maureen G. Friedman, Bella Dvoskin, MaijaLeinonen, Bella Ohana, Ida Boldur. A comparative study of the etiology of adult upper and lower respiratory tract infections in the community. Diagnostic Microbiology and Infectious Disease, Volume 42, Issue 1, January 2002, Pages 21-28, ISSN 0732-8893 Macfarlane J, Holmes W, Gard P, Macfarlane R, Rose D, Weston V, Leinonen M, Saikku P, Myint S. Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community. Thorax 2001;56:109-114 doi:10.1136/thorax.56.2.109 Gencay, M., Roth, M., Christ-crain, M., Mueller, B., Tamm, M., & Stolz, D. Single and multiple viral infections in lower respiratory tract infection. (2010). Respiration, 80(6), 560-7. doi:http://dx.doi.org/10.1159/000321355 W. Paul Glezen, M.D. Influenza Control. N Engl J Med 2006; 355:79-81July 6, 2006DOI: 10.1056/NEJMe068114 William P. Goins, H. Keipp Talbot, and Thomas R. Talbot. Infection Prevention and Control in the Hospital Health Care–Acquired Viral Respiratory Diseases. Infectious Disease Clinics of North America, 2011-03-01, Volume 25, Issue 1, Pages 227-244. RESULTS A total of 1,256 patients were enrolled in the study, consisting of 109 patients with Acute Bronchitis, 346 Acute Exacerbation of Chronic Obstructive Pulmonary Disease, 531 Community Acquired Pneumonia, and 270 Health-care Associated Pneumonia (shown in figure 1). Of these Influenza virus was isolated in 45 of the acute bronchitis patients (41%), 52 of Acute Exacerbation of COPD patients (15%), 80 of the CAP patients (15%), and 32 of the HCAP patients (12%).(shown in figure 2)



















