Download
1 / 53
530 likes | 565 Views
Explore the pathology of cardiac insufficiency & vascular tone. Learn about the classifications, etiology, and clinical manifestations of cardiac insufficiency and coronary blood circulation disorders. Lecturer: PhD Ivanytsa A. in Vinnytsya National Pirogov Memorial Medical University

E N D
CARDIAC INSUFFICIENCYPATHOLOGY OF VASCULAR TONE Lecturer: PhD Ivanytsa A. VinnytsyaNational Pirogov Memorial Medical University Pathophysiology Department
. • Insufficiency of blood circulation of is the state when the cardio-vascular system can not provide organs and tissues of an organism with necessary amount of blood
Cardiac insufficiency is the pathological condition characterized by inability of the heart to provide blood supply of organs and tissues in accordance with their necessities.
Classification of cardiac insufficiency 1.According to clinical course cardiac insufficiency is divided into: • acute; • chronic. 2.According to clinical manifestations intensity cardiac insufficiency is dividedinto: • compensated; • decompensated.
3.According to injured parts of the heart cardiac insufficiency is divided into: • left ventricle cardiac insufficiency; • right ventricle cardiac insufficiency; • total cardiac insufficiency.
4.According to pathogenesis cardiac insufficiency is divided into: • cardiac insufficiency due to overload of the heart: -overload of heart by volume (reasons: heart disease with valvular insufficiency, hypervolemia); -overload of heart by resistance (reasons: heart disease with valvular stenosis, arterial hypertension);
cardiac insufficiency due to damage of myocardium (reasons: arrhythmias, myocarditis, myocardiopathys); • cardiac insufficiency due to violation of the coronary blood circulation (reasons: atherosclerosis, tromboembolism or spasm of coronal vessels); • cardiac insufficiency due to the injury of pericardium (acute and chronic pericarditis, cardiac tamponade); • mixed form.
Cardiac insufficiency due overload of the heart 1.overload by blood volume - emerges when the inflow of the blood to a definite part of the heart is increased: • hypervolemia • valvular insufficiency
2. overload by resistance - emerges when the resistance to the heart outflow is increased and develops at: • arterial pressure increase • valvular stenosis (the left ventricle overload develops at aortal stenosis, at mitral stenosis - left atrium, at pulmonary valve artery stenosis - right ventricle, at tricuspid stenosis - right atrium).
Cardiac insufficiency due to damage of the myocardium Etiology: • arrhythmias - related to the damage of the heart conducting system; • myocarditis - related to the damage of myocardium of inflammatory origin (e.g., bacteria, viruses, fungi, allergens, toxic factors); • myocardiopathys - related to the congenital or acquired damage of myocardium noninflammatory origin (e.g., alcohol, anemia, intoxication, hypoxia).
Cardiac insufficiency due to violation of the coronary blood circulation Insufficiency of coronary blood circulation is the pathology which is characterized by inability of coronary vessels to supply blood to the heart in accordance with its requirements.
Coronary heart disease (CHD) is illness which develops as a result of absolute insufficiency of coronary circulation and characterized by the myocardium damage. Etiology: • atherosclerosis of coronary vessels; • thromboembolism of coronary vessels; • primary thrombosis or embolism of coronary vessels • spasm of coronary vessels • inflammation in the coronary vessels ,(e.g., rheumatism); compression of coronary vessels (e.g., scars, tumors, ligature).
Main clinical forms of CHD: 1.Stenocardia (angina pectoris)is characterized by attacks of brief (to 20 min) acute myocardium ischemia which are accompanied by a pain syndrome, sense of fear, vegetative reactions, pain is relieved by nitroglycerine 2.the preceding infarction state is the acute focal myocardium dystrophy which develops during myocardial ischemia from 20 to 40 min;
3.the myocardial infarctionis the necrosis of myocardium, caused by coronary circulation violation. Emerges at a reversible ischemia continued over 40-60 min, or at irreversible coronary circulation violation , «-» effect of nitroglycerine 4.cardiosclerosisisthe sclerotic changes of cardiac muscle. It can be diffuse (atherosclerotic cardiosclerosis) and focal (postinfarction atherosclerotic cardiosclerosis).
Clinical syndromes which characteristic for the myocardial infarction • pain; • acute cardiac insufficiency - develops at the injury of large areas of myocardium and characterized by the cardiac asthma syndrome, pulmonary edema or cardiogenic shock; • arrhythmia - possibly development of all types of arrhythmias at myocardial infarction. Appearance of ventricular fibrillation is the most dangerous; • reperfusion syndrome; • resorption - necrotizing syndrome.
Clinical signs which characteristic for the myocardial infarction • Unbearable pain behind the breastbone with irradiation in the left shoulder, armand others. • The skin is pale, cold. • His face covered with sweat, with a bluish tinge. • Pulse is thready, weak filling, frequent, sometimes arrhythmic. • Pulmonary edema.
MI LaboratoryDiagnostics:Elevated level of enzymes !!!!: (damage of cell membranes)↑ CPK (creatine phosphokinase)↑ AST, ALT↑ LDH1,22. ↑ troponins 3. neutrophilic leukocytosis, left shift of leukogramm4. ↑ ESR
ECG changes 1. Zone Necrosis - pathological Q wave or QR, QRS, QS 2. Zone damage - domedlifting ST, which is a sign of acute stage and discordant changes of the opposite parts;3. Zone of ischemia - negative, high, spiky T.
Сomplicationsof myocardial infarction Reperfusion syndrome emerges as a result of re-establishment blood flow in the area of myocardial ischemia over 40 min ischemia duration. The pathogenetic basis of the reperfusion syndrome is so-called «oxygen paradox», because of the lipid peroxidation activating and plenty of free radicals formation which damage the cellular membranes.
Cardiogenic shock emerges as a result of the acute falling of the pumping ability of the heart. Etiology: • myocardial infarction; • congestive heart failure; • cardiomyopathy; • pulmonary edema; • cardiac tamponade; • ineffective pumping due to cardiac dysrhythmias and from acute disruption of valvular function.
Pathogenesis of cardiogenic shock: 1. The initial ↓ of arterial pressure 2. Compensatory spasm of arterioles 3. Secondary ↓ of arterial pressure 4. Terminal changes
Resorption - necrotizing syndromeat the myocardial infarction is the outcome of the entry of necrotic products of myocardial disintegration into blood Signs: • fever; • neutrophilic leukocytosis; • increase of ESR; • appearance in the blood of enzymes from damaged cardiomyocytes (creatine kinase, AST, LDH;)
Dressler's syndrome - develops as a result of autoantibodies’ production on the changed myocardium proteins and characterized by serous membranes inflammationnism - polyserositis (c.g., pericarditis, pleurisy, peritonitis).
Cardiac insufficiency due to pathology of the pericardium Etiology: pathology of pericardium, as a result heart’s work is violated during a diastole (e.g., exudate or transudate accumulation in the cavity of pericardium, acute cardiac tamponade). Clinical signs: • arterial hypotension; • diminishing of ECG wave voltage; • enlargement of the heart.
Acute cardiac tamponade Acute cardiac tamponade is rapid accumulation of liquid in the cavity of pericardium because of hemorrhage at the wound or cardiac rupture, or at quickly developing pericarditis
Mechanisms of compensation of the heart's work urgent mechanisms of compensation: • the heterometric mechanism provides compensation at the cardiac overload by a volume (reasons: heart disease with valvular insufficiency, hypervolemia). Its essence consists in the increase of force of the heartbeats in the case of entrance to the heart of bigger blood volume (а law of Frank-Starling’s)the homeometric mechanism provides compensation at the cardiac overload by resistance (reasons: heart disease with valvular stenosis, arterial hypertension). Its essence consists in the increase of force of the heartbeats in case of the increase of resistance to blood flow. • tachycardia provides constant level of the minute blood volume.
Mechanism of long duration adaptation of the heart is the myocardial hypertrophy. myocardial hypertrophy according to F. Meerson: • myocardial hypertrophy in sportsmen - develops at periodically increasing loadings; it's characterized by the increase of all parts of the heart (myocardiocytes,vessels and nerves) • compensotory myocardial hypertrophy: 1.hypertrophy due to overloads (develops at the cardiac insufficiency, arterial hypertension); 2. hypertrophy due to the damage (e.g., atherosclerosis, myocarditis).
Stages of compensatory heart hypertrophy development of according F. Meerson: • emergency stage • stage of complete hypertrophy and relatively proof hyperfunction • stage of gradual exhaustion and progressive cardiosclerosis
Dilatation of myocardium • Tonogenic dilatation - this is expansion of heart cavities, that is accompanied by the increase of stroke volume of blood. Develops as a result of activating of heterometric mechanism of provides compensation. • Myogenic dilatation arises up at the dystrophic changes of myocardium. It is accompanied by expansion of cavities of heart and decrease of force of cardiac contractions. Arises up during decompensation of cardiac insufficiency.
Indicators hemodynamic: • blood flow velocity; • circulatory blood volume • stroke volume of the heart • cardiac output • heart rate • cardiac index • Arterial pressure • venous pressure • total peripheral resistance • rate of oxygen utilization
The indices of hemodynamics change during cardiac decompensation: • cardiac output diminishes; • under the left ventricle cardiac insufficiency: 1)arterial hypotension in the systemic circulation; 2)common peripheral resistance increases; 3)hypertension of the pulmonary circulation, which leads to the lungs edema; • under the right ventriclecardiac insufficiency 1) hypotension of the pulmonary circulation; 2) resistance of the pulmonary circulation vessels increases hereupon; 3)central venous pressure increases which leads to the congestion in the systemic circulation; • the circulatory blood volume increases.
Clinical symptoms of cardiac insufficiency: • circulatory hypoxia; • shortness of breath because of acidosis and lungs edema; cyanosis because of venous hyperemia; • edema (under the right ventricle cardiac insufficiency edema develops on the lower extremities, under the left ventricle cardiac insufficiency develops lungs edema); • portal hypertension and cardiac cirrhosis develops under the right ventricle cardiac insufficiency; • ABB violations: metabolic lactate acidosis because of the lactic acid accumulation and gas alkalosis because of shortness of breath; secondary hyperaldosteronism due to activating of the renin-angiotensin- aldosteron system and because of diminishing of aldosteron disintegration in the liver • Cyanosis (↑ concentration of reduced hemoglobin ).
Acute cardiac insufficiency develops quickly, at the surplus loading on a heart, when all compensatory mechanisms are not corrected with it , e.g., at the myocardium infarction and its complications (cardiogenic shock, tamponade of heart), at arrhythmias (fibrillation of heart, paroxismal tachycardia, complete atrioventricular blockade), acute pericarditis, myocarditis, embolism of pulmonary artery.
Clinical manifestations 1) cardiac asthma,2) pulmonary edema 3) cardiogenic shock.
Chronic (stagnant) cardiac insufficiency develops gradually, mainly as a result of metabolic violations in myocardium at protracted hyperfunction of heart or different types of myocardium damage (e.g., arterial hypertension, cardiomyopathys, and others).
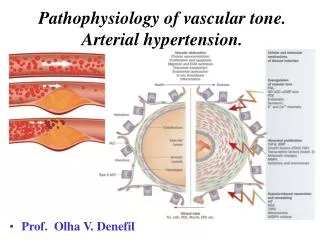
Normal AP:-100 - 120 / 70-80 mm Hg (17 - 20 ) -120 - 140 / 80-90 mm Hg (21 - 60) Arterial hypertension is the increase of systolic pressure more than I40mni Hg and diastolic more than 90mm Hg.
Classification of arterial hypertension : • primary hypertension (essential or idiopathic hypertension) appears to be a familial disease of unknown etiology • secondary hypertension develops secondary to another disease; • hypertensive crisis is a sudden acute elevation in arterial blood pressure • isolated systolic hypertension refers to an elevation in systolic blood pressure greater than 140 mm Hg without a concurrent elevation in diastolic blood pressure (elderly persons)
II. The type of high blood pressure: 1. Systolic. 2. Diastolic. 3. Mixed. ІІІ. The value of the cardiac output (cardiac output):Hyperkinetic: ↑cardiac output (↑ circulating blood volume).Hypokinetic: ↑vascularresistance(hypertension) - ↑ diastolic blood pressure.Eukinetic. IV. The level of renin:hyperreninemic.Normoreninemic.Hyporeninemic
Etiology: • Primary hypertensionresults from unknown causes, it accounts for 80% of hypertension cases. • Secondary hypertension10% of hypertension cases: • renal diseases-may cause accelerated renin release, which, in turn, elevates blood pressure; • Cushing's syndrome, which causes accumulation of extracellular sodium and water; • primary aldosteronism, which causes accumulation of extracellular sodium and water; • hypothyroidism and hyperthyroidism • coarctation of the aorta • excessive alcohol ingestion and prolonged use of oral contraceptives.
Risk factors of essential hypertension: main factors: • psycho-emotional overload (chronic stress situations) • Excessive consumption of salt, • hereditary predisposition, • low body weight at birth • male sex; middle age ; black color of skin; hypodynamia; • insulin resistance; • urban population,bad habits (e.g., cigarette smoking).
Pathogenesis of primary (essential) hypertension • Dysregulatory theory - violations of regulatory mechanisms of arterial vessels tone. There are two phases: 1. Hyperkinetic 1 stage: activation of the sympathetic and adrenal system under the action of stress factors 2 stage: activation of the rennin-angiotensin-aldosteron system 3 stage: activation of aldosteron and vasopressin systems
Pathogenesis of primary (essential) hypertension 2. Hypokinetic- is characterized by the irreversible structural changes of compession and resistance vessels, peripheral vascular resistance and arterial vessels tone grows as a result constantly. The main significance has following factors: • constant spasm of arterioles; • hypertrophy of smooth muscles; • atherosclerosis and substitution of smooth muscles by connective tissue.
Pathogenesis of primary (essential) hypertension • Membrane theory is the hereditarily conditioned violation of ionic pumps of membranes of smooth muscles fibers: • defect of Ca2+- pump- this leads to the development of permanent contraction and the increase of peripheral vascular resistance. • decrease work of Na -K –pump - the outcome is the thickening of vessel’s wall and diminishing of diameter of vessels increase of sensitization to the action of catecholamine, damage and necrosis of cells, atherosclerosis).
Arterial hypotension is the decrease of systolic pressure less than 100 Hg and diastolic less than 60 mm Hg. Kinds: • Physiological (it is not accompanied by the symptoms of illnesses). • Pathological: А) acute (shock and collapse) B) сhronic(primary and secondary):
secondary (symptomatic) arterial hypotensionis a result of acute and chronic heart diseases (congenital heart diseases, myocarditis, infarction of myocardium); brain diseases, lungs diseases (croupous pneumonia), liver diseases (hepatitis, mechanical jaundice), blood diseases (anemia), endocrine diseases (Addison’s disease) and intoxications; • primary arterial hypotensiondevelops at patients with neurocirculatory dystonia of hypotension type (essential, primary, idiopathic hypotension).
Collapse • Collapse is acute vascular insufficiency which is characterized by the acute dicrease of arterial vessels tone and central- venous pressure and diminished circulatory blood volume. Types of collapse: • toxic and infectious collapse, - develops at intestinal infections (dysentery, salmonellosis) due to the action of endotoxins (after death of microorganisms). • hemorrhagic collapse - arises up at acute massive bleeding and related to the rapid decrease, of volume of circulatory blood • pancreatic collapse - at the mechanical trauma of pancreas or acute pancreatitis and liberation of tripsin in blood • orthostatic collapse - arises up in acute transition from horizontal position to vertical position • anoxic - arises up at the rapid decrease of partial pressure of oxygen in air, as a result of anoxemia develops, decrease of vessels tone
Pathogenesis of collapse The decrease of volume of circulatory blood and vessels’ tone leads to the decrease of venous return to the heart, decrease of cardiac output decrease of both arterial and venous pressure and disturbance of tissues perfusion and metabolism, which leads to the brain hypoxia.
Atherosclerosis is pathology of vascular wall, which characterize by the sedimentation of lipids, elements of blood, calcium and connecting tissue in its internal membrane (tunica intima).