Download
1 / 35
350 likes | 485 Views
Ontology and Referent Tracking for Neurodegenerative Disorders. Dr. Werner Ceusters European Centre for Ontological Research Saarland University, Saarbrücken, Germany. Part I. Neurodegenerative disorders: modern history. Examples of neurodegenerative diseases.

E N D
Ontology and Referent TrackingforNeurodegenerative Disorders Dr. Werner Ceusters European Centre for Ontological Research Saarland University, Saarbrücken, Germany
Examples ofneurodegenerative diseases • Involving the central nervous system: • Alzheimer's Disease • Parkinson Disease • ALS (Lou Gehrig's Disease) • Frontal Temporal Dementia • Huntington's Disease • Cerebellar Ataxias • Hereditary Spastic Paraplegias • Involving the peripheral nervous system: • Charcot-Marie Tooth Hereditary Neuropathies • Muscular Dystrophy.
Some disease characteristics • Neurodegeneration is a major element. • But some disorderswith ND are not usually classified as degenerative e.g. multiple sclerosis, epilepsy, some inborn errors of metabolism, schizophrenia, and even tumours. • selective, at least initially, for a particular neuronal pool • both genetic and environmental risk factors play a part in the etiology • a long run-in period until sufficient protein accumulates, followed by a cascade of symptoms over 2-20 years, with increasing disability leading to death A. Williams. Defining neurodegenerative diseases. BMJ 2002;324:1465-1466 ( 22 June )
Wide range of phenotypes in same category, e.g. cerebellar ataxias (SCA) • SCA 1: hypermetric saccades and hyperreflexia. • SCA 2: reduced velocity of saccadic eye movements, areflexia and changes similar to those seen in olivopontocerebellar atrophy on brain imaging. • SCA 3: protruded eyes, muscle fasciculations, spasticity, chorea, gaze-evoked nystagmus, parkinsonism and peripheral neuropathy. • SCAs 5, 6, 10 and 11: pure cerebellar signs. • SCA 7:macular degeneration. • SCA 8:mild sensory neuropathy, late-onset spasticity. • SCA 10: seizures with ataxia. • SCA 12: head and hand tremors. • SCA 17: Intellectual deterioration and dysphagia. T.E. King. Molecular diagnosis of adult neurodegenerative diseases and movement disorders. April 2005. http://www.bioethics-singapore.org/resources/pdf/GeneticTestingMovementDisorders_tanek.pdf
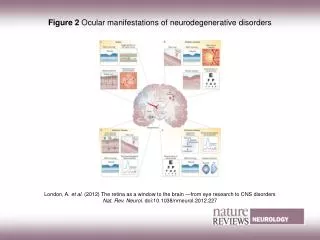
Histopathological phenomenain some central NDs L. Bertram and R.E. Tanzi. The genetic epidemiology of neurodegenerative disease. J. Clin. Invest. 115:1449-1457 (2005).
Multi-factorial with cross-relations, e.g. genetic epidemiology of Alzheimer L. Bertram and R.E. Tanzi. The genetic epidemiology of neurodegenerative disease. J. Clin. Invest. 115:1449-1457 (2005).
Main research epochs • Early 1900 • Microscopic study of stained tissues • Alzheimer, Lewy, Pick, ... • NDs classified as clinicopathological entities • Last decade: • Molecular genetics and molecular biology • Advanced functional and sequential imaging • NDs classified by means of pathological biochemical pathways
Research purposes for ND • characterize the clinical, laboratory, and pathological phenotypes of the various disorders included in this category; • identify and clone genes directly causing or functioning as risk factors for these disorders; • understand basic mechanisms underlying the biochemical and molecular pathogenesis of these disorders; • Find application to treatment and prevention
Research purposes froman –omics perspective • understand the normal functions of genes and proteins involved in neurodegenerative diseases, • characterize their role in pathogenic disease mechanisms, • model their functions in animals, • explore their roles in the diagnosis, treatment and prevention
Technical strategy foranalysing ND pathogenesis • identify pathogenic genes • by positional cloning, • by cloning genes that encode proteins involved in the disease, • or by combining the two approaches; • find pathogenic mutations; • model and study the disease • in cells by transfection and • in mice by transgenesis D. L. Price, S. S. Sisodia, D. R. Borchelt, Science 282, 1078 (1998)
E.g.: ‘positional cloning’ • identify large multigenerational families with a long history of carrying the disorder • determine linkage with polymorphic genetic markers • look for cytogenetic rearrangements associated with the disease • isolate overlapping DNA clones from the region • identifying the gene that is responsible
Another strategy for ND gene detection L. Bertram and R.E. Tanzi. The genetic epidemiology of neurodegenerative disease. J. Clin. Invest. 115:1449-1457 (2005).
New NDs are discovered • a previously unrecognized adult-onset dominantly inherited ND that affects the basal ganglia associated with iron accumulation. • Phenotype: • extrapyramidal symptoms and low ferritin serum levels. • lesions in the globus pallidus with abundant spherical inclusions containing aggregates of ferritin and iron. • axonal swellings throughout the brain • organs such as the pancreas, liver, and heart that are typically affected in iron accumulation disease, appear to function normally Curtis ARJ, Fey C, Morris CM, et al. Mutation in the gene encoding ferritin light polypeptide causes dominant adult-onset basal ganglia disease. Nature Genetics 2001; 28: 350-354.
Intermediate conclusions • NDs are challenging with respect to ‘reality representation’ • Involve entities of diverse nature • ‘true’ nature of some entities not yet understood • Type of relationships unclear
Ontology • ‘Ontology’: the study of being as a science • ‘An ontology’ : a representation of some pre-existing domain of realitywhich • (1) reflects the properties of the objects within its domain in such a waythat there obtains a systematic correlation between realityand the representation itself, • (2) is intelligible to a domain expert • (3) is formalized in a way that allows it to support automatic information processing • ‘ontological’ (as adjective): • Within an ontology. • Derived by applying the methodology of ontology • ...
Need for widely acceptedTop Level Ontology (TLO) • TLO: an ontology that describes by means of theories or specifications the most general, domain-independent categories of reality such as time, space, inherence, instantiation, identity, processes, events, attributes, relations, ... • Ongoing efforts: • BFO • DOLCE • SUMO
Need for widely acceptedBiomedical Domain Ontology (BMO) • domain ontology: • an ontology that describes the most general categories within a specific domain, using the framework of the top level ontology. In our case: the domain is biomedicine. • Where a top level ontology describes entities such as objects and processes, a biomedical domain ontology: • describes entities such as genes and insulin, and transcription and hormon secretion. • further classifies these entities within the framework of the top level ontology, thereby adding new descriptive elements that are relevant at that level of reality.
Essential (and missing) components for a biomedical domain ontology • Ontology for functions and processes • levels of granularity for functions: • localizing functions and processes to understand their mutual relationships: • functional states of molecules • Ontology for anatomical levels of granularities • levels of granularity based on grains and structure • determination of parthood relations across entities in different levels of granularity • Pathophysiology ontology • Dependence relations between physiological entities and pathology • Determination of parthood relations for pathological entities • An upper ontology for health information stored in public health information databases
Links to ongoing efforts • Use BMO: • To make more DB semantics explicit and formal • to make the various databases semantically interoperable at both structure and content level.
Example:KEGG Pathway Database onNeurodegenerative Disorders • Alzheimer's disease • Parkinson's disease • Amyotrophic lateral sclerosis (ALS) • Huntington's disease • Dentatorubropallidoluysian atrophy (DRPLA) • Prion disease
The missing link • ‘From genotype to phenotype’ • Most DBs contain data without reference to particular patients • Some DBs (usually not publicly accessible) just have snapshots of correlations • No DBs provide a dynamically growing pool of data about interrelated patient phenomena • Note: • NOT “interrelated data” • Relationships between data are distinct from relationships amongst the entities the data are about • The right approach: Referent Tracking
Referent Tracking ... • Corrects the overemphasis on data and information and too little attention to reality: • “data modelling” • “information modelling” • Does right what the “Object Oriented” model claims to do right. • objects are said to be those things that exist in reality • But: ‘The object-oriented model is based on a collection of objects’ • An object contains values stored in instance variables within the object. • Unlike the record-oriented models, these values are themselves objects.
PtID Date ObsCode Narrative 5572 5572 298 5572 5572 5572 298 2309 47804 5572 5572 12/07/1990 01/04/1997 22/08/1993 22/08/1993 01/04/1997 12/07/1990 21/03/1992 03/04/1993 04/07/1990 17/05/1993 04/07/1990 26442006 2909872 9001224 26442006 9001224 58298795 26442006 9001224 79001 79001 81134009 Essential hypertension closed fracture of shaft of femur Fracture, closed, spiral closed fracture of shaft of femur Accident in public building (supermarket) Other lesion on other specified region closed fracture of shaft of femur Essential hypertension Accident in public building (supermarket) Closed fracture of radial head Accident in public building (supermarket) 5572 04/07/1990 79001 Essential hypertension 0939 24/12/1991 255174002 benign polyp of biliary tract 2309 21/03/1992 26442006 closed fracture of shaft of femur 0939 20/12/1998 255087006 malignant polyp of biliary tract A look at the database: Use of SNOMED codes for ‘unambiguous’ understanding How many numerically different disorders are listed here ? * How many different types of disorders are listed here ? * How many disorders have patients 5572, 2309 and 298 each had thus far in their lifetime ? * * cause, not disorder
PtID Date ObsCode Narrative 2309 298 5572 298 5572 5572 5572 47804 5572 5572 5572 01/04/1997 04/07/1990 04/07/1990 22/08/1993 12/07/1990 22/08/1993 12/07/1990 01/04/1997 21/03/1992 03/04/1993 17/05/1993 79001 26442006 9001224 81134009 26442006 26442006 58298795 2909872 9001224 79001 9001224 Accident in public building (supermarket) Closed fracture of radial head closed fracture of shaft of femur Fracture, closed, spiral closed fracture of shaft of femur closed fracture of shaft of femur Other lesion on other specified region Accident in public building (supermarket) Essential hypertension Accident in public building (supermarket) Essential hypertension Would it be easier if youcould see the code labels ? 5572 04/07/1990 79001 Essential hypertension 0939 24/12/1991 255174002 benign polyp of biliary tract 2309 21/03/1992 26442006 closed fracture of shaft of femur 0939 20/12/1998 255087006 malignant polyp of biliary tract
Proposed solution:Referent Tracking • Purpose: • explicitreference to the concrete individual entities relevant to the accurate description of each patient’s condition, therapies, outcomes, ... • Method: • Introduce an Instance Unique Identifier(IUI) for each relevant individual (= particular, = instance). • Distinguish between • IUI assignment: for instances that do exist • IUI reservation: for entities expected to come into existence in the future
PtID Date ObsCode Narrative IUI-001 5572 5572 2309 5572 5572 5572 298 5572 298 5572 47804 03/04/1993 01/04/1997 04/07/1990 04/07/1990 12/07/1990 12/07/1990 21/03/1992 01/04/1997 17/05/1993 22/08/1993 22/08/1993 26442006 81134009 26442006 9001224 9001224 79001 58298795 79001 2909872 26442006 9001224 Accident in public building (supermarket) closed fracture of shaft of femur Other lesion on other specified region closed fracture of shaft of femur Essential hypertension Accident in public building (supermarket) Closed fracture of radial head Essential hypertension closed fracture of shaft of femur Fracture, closed, spiral Accident in public building (supermarket) IUI-001 IUI-001 IUI-007 5572 04/07/1990 79001 IUI-005 Essential hypertension 0939 24/12/1991 255174002 IUI-004 benign polyp of biliary tract 2309 21/03/1992 26442006 IUI-002 closed fracture of shaft of femur IUI-007 IUI-005 IUI-007 IUI-012 IUI-005 0939 20/12/1998 255087006 IUI-004 malignant polyp of biliary tract No confusion withexplicit references IUI-003
Essentials of Referent Tracking • Generation of universally unique identifiers; • deciding what particulars should receive a IUI; • finding out whether or not a particular has already been assigned a IUI (each particular should receive maximally one IUI); • using IUIs in the EHR, i.e. issues concerning the syntax and semantics of statements containing IUIs; • determining the truth values of statements in which IUIs are used; • correcting errors in the assignment of IUIs.
Architecture of aReferent Tracking System (RTS) • RTS: system in which all statements referring to particulars contain the IUIs for those particulars judged to be relevant. • Ideally set up as broad as possible: • some metrics: • % of particulars referred to by means of IUI • % of HCs active in a region • Geographic region • functional region: defined by contacts amongst patients • % of patients referred to within a region • Services: • IUI generator • IUI repository: statements about assignments and reservations • Referent Tracking ‘Database’ (RTDB): index (LSID) to statements relating instances to instances and classes
Ultimate goal Ontology continuant disorder person CAG repeat EHR Juvenile HD #IUI-1 ‘affects’ #IUI-2 #IUI-3 ‘affects’ #IUI-2 #IUI-1 ‘causes’ #IUI-3 ... Referent Tracking Database