Download
1 / 63
640 likes | 816 Views
Conventional & Digital Chest Radiography & Computed Tomography in Occupational Lung Diseases. John E. Parker, M.D. Pulmonary & Critical Care Medicine West Virginia University Morgantown, WV USA 11 th Annual Congress Turkish Thoracic Society 2008 24 Nisan 2008. Presenter Disclosures.

E N D
Conventional & Digital Chest Radiography & Computed Tomography in Occupational Lung Diseases John E. Parker, M.D. Pulmonary & Critical Care Medicine West Virginia University Morgantown, WV USA 11th Annual Congress Turkish Thoracic Society 2008 24 Nisan 2008
Presenter Disclosures John E. Parker, M.D. “No relationships to disclose” The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Thanks for the privilege • Present and attend the 11th TTS in Antalya • Meet colleagues for professional scientific interactions and renewing, making, and maintaining personal friendships • The knowledge that a forest is being grown because of the Turk Toraks Dernegi
Goals of Presentation- Imaging • Review the advantages and limitations of chest radiographic imaging for occupational respiratory disorders • Review the utility of computed tomography in the study and evaluation of dust related lung diseases • Look at some images of silica- and asbestos- related diseases on both CXR and HRCT • Review the ILO guidelines used for grading or scoring pneumoconiosis & introduce an HRCT scoring system • Make a pitch for the wide acceptance of digital radiography • Look at some wildlife photos and paintings
Roles for Chest Radiography in Clinical Medicine • CXR is an important and classic tool for evaluating pulmonary disease – both for occupational and for non- occupational respiratory diseases • Useful in clinical care, assisting in both the diagnosis of disease & for the evaluation of response to therapeutic interventions • Especially helpful in the diagnosis of infectious, neoplastic, and interstitial lung diseases
Chest Radiography in Dust Exposed Workers • Chest radiography has been useful tool in screening and surveillance of dust exposed workers • Major role in establishing dose or exposure response relationships, what is safe? • Although a helpful tool, improvement is possible • Documents failures of dust control
Diego Rivera: El vendedor de floresDust diseases impose a heavy burden on workers, their families, and on societies all over the world
Occupational Respiratory Disease Spectrum Chest imaging only helpful in some diseases
Limitations of Chest Radiographic Imaging • Imperfect tool, not diagnostic gold standard • Airway disorders not well evaluated by imaging • Functional impairment not well evaluated or assessed • Imaging cannot provide certainty about the etiology of observed findings due to limited lung response patterns – but rather images generate differential diagnostic considerations
2002 Revision of the ILO Guidelines for Radiology of the Pneumoconiosis • Introduces new written guidelines describing profusion, size, shape, location of small opacities • Introduces more 2 letter symbols for other findings • Includes clarifications of ambiguities of the 1980 ILO guidelines especially for pleural abnormalities • Introduces new sectional standard radiographs – an optional 14 film standard set • Correction of pleural standard film labeling & provides an example of diffuse thickening
What other imaging techniques do we have to take a good hard look at the lungs and pleura
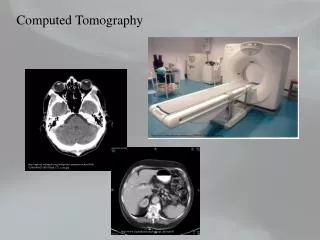
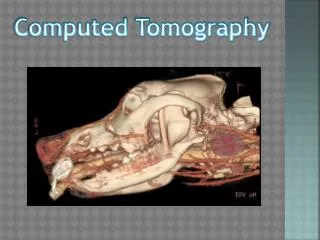
What About A Role for Computed Tomography • Becoming more widely available • Provides images with exquisite detail of pulmonary parenchyma and other structures • HRCT and CT has excellent anatomical correlation with pathological findings • Not currently a universally accepted “ILO system” for HRCT or CT
HRCT and CT Advantages • Visualize parenchyma even when pleural shadows are competing on the PA image • See pleural surfaces in more detail, clearly superior to PA radiograph for recognition • Identify other diseases, emphysema or cancer • In some cases may clarify presence or absence of abnormalities on low profusion Posterior-Anterior Chest films
Limitations of HRCT and CT • Cost for scanners and operation prohibitive for some nations and some settings • Radiation dose concerns • Not recommended for screening • Not a panacea for drawing the line between disease and health • Cannot always distinguish occupational from non-occupational etiology of findings
HRCT Classification Standardization Project • Multinational effort--Japan, US, Germany, Finland, France, Belgium, Brasil, and UK • Similar, but distinct from the ILO chest radiographic classification system • Standardizes imaging parameters • Introduces comparison or reference films • Features a standardized reading sheet
Jack Parker: CT-Classification of Occupational and Environmental Respiratory Diseases: R0/Irr0
CT-Classification of Occupational and Environmental Respiratory Diseases: R0/Irr0
CT-Classification of Occupational and Environmental Respiratory Diseases: R0/Irr0
CT-Classification of Occupational and Environmental Respiratory Diseases: R0/Irr0 Calcified plaques
CT-Classification of Occupational and Environmental Respiratory Diseases: RGr2Q
CT-Classification of Occupational and Environmental Respiratory Diseases: RGr2Q
CT-Classification of Occupational Respiratory Diseases: AX or coalescence
CT-Classification of Occupational Respiratory Diseases: Large opacity B size
CT-Classification of Occupational and Environmental Respiratory Diseases: IrrGr1
CT-Classification of Occupational and Environmental Respiratory Diseases: IrrGr2
CT-Classification of Occupational and Environmental Respiratory Diseases: IrrGr2
CT-Classification of Occupational and Environmental Respiratory Diseases: Pleura - parietal type, width b
CT-Classification of Occupational and Environmental Respiratory Diseases: Pleura - parietal and visceral type, width c
CT-Classification of Occupational Respiratory Diseases: FP-Extrapleural fat
CT-Classification of Occupational and Environmental Respiratory Dis: CANCER
CT-Classification of Occupational Respiratory Diseases: Emphysema Grade 3
CT-Classification of Occupational Respiratory Diseases: Honeycombing grades 1-3 HC Grade 3 HC Grade 2 HC Grade 1
CT-Classification of Occupational Respiratory Diseases: Rounded Atelectasis
Limitations of HRCT and CT • Cost for scanners and operation prohibitive for some nations and some settings • Radiation dose concerns • Not recommended for screening, but is recommended for individual patient care • May not be as useful for silica related diseases as for asbestos related diseases
Limitations of HRCT and CT • HRCT is not recommended for large screening projects, but can be important for individual patient care • Not the magic solution for drawing the line between disease and no disease or health • HRCT still has the same challenge as the chest radiograph to separate low level profusion of disease at the “0/1 vs. 1/0” boundary • HRCT cannot always distinguish occupational from non- occupational etiology of findings
Roles for HRCT - I • HRCT is a useful supplement but not a replacement for chest radiography • HRCT is helpful in difficult cases where CXR is equivocal for pneumoconiosis • HRCT is useful when lung function is discordant with the radiograph