Download
1 / 23
230 likes | 334 Views
Hope in the Pipeline The Search for New TB Vaccines. Peg Willingham Aeras Global TB Vaccine Foundation “Journalist to Journalist” National Press Foundation December 4, 2009 Cancun, Mexico. Invention of Bacille Calmette-Guérin (BCG) Vaccine. By Calmette & Guérin 1908-1921

E N D
Hope in the PipelineThe Search forNew TB Vaccines Peg Willingham Aeras Global TB Vaccine Foundation “Journalist to Journalist” National Press Foundation December 4, 2009 Cancun, Mexico
Invention of Bacille Calmette-Guérin (BCG) Vaccine By Calmette & Guérin 1908-1921 No new TB vaccine in almost 90 years
BCG Vaccine Efficacy • BCG is one of the most widely used vaccines in the world, yet TB remains the second leading cause of infectious disease deaths • Prevents some severe forms of TB in children, saves 40,000 to 70,000 children a year • Fails to prevent pulmonary tuberculosis, the most common form, and TB in adults (nearly two million people die each year)
Tuberculosis: TB Vaccine Too Dangerous for Babies With AIDS Virus, Study Says July 2, 2009 – The vaccine against tuberculosis that is routinely given to 75 percent of the world’s infants is too risky to give to those born infected with the AIDS virus, says a new study published by the World Health Organization. It recommended that vaccination be delayed until babies can be tested.
WHO Guidance on BCG • World Health Organization (WHO) changed guidelines in 2007 • BCG is not recommended for infants known to be infected with HIV, due to increased risk of disseminated BCG disease (one percent of infants with HIV who receive the vaccine get disseminated BCG, 75 percent die) • Difficult to implement in practice
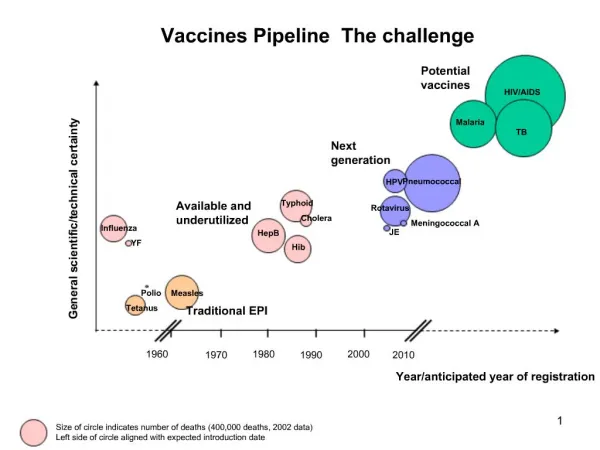
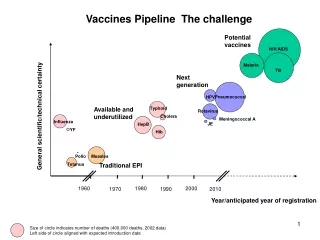
Potential of a New TB Vaccine • Eliminate TB as a public health threat, in line with global targets (<1 case/million), in conjunction with new drugs and diagnostics • Safe and effective in preventing TB in children, adolescents and adults, including people with HIV • Protect against all forms of TB – including MDR and XDR • Reduce the cost and burden of TB on patients, health care systems and national economies
Block Initial Infection Prevent Latent Infection Prevent Early Disease Prevent Reactivation Disease
All age groups * *Pre-exposure vaccine with additional effects that reduce the lifetime risk of developing disease in slow progressors by half to about 2.5% and the infectiousness of the smear-positive and smear-negative cases by half. Abu-Raddad, Sabatelli, Achterberg, Sugimoto, Longini, Dye and Halloran
Aeras Global TB Vaccine Foundation Mission To develop new, more effective TB vaccines and ensure their availability to all who need them Goals • A more effective, safe and affordable TB vaccine by 2016 • Identify correlates and surrogate markers of vaccine induced protection • Develop second generation TB vaccines with increased potency and broader protection
Aeras Global Vaccine Development Partners Aeras Academia Oxford University, United Kingdom South African TB Vaccine Initiative (SATVI), South Africa St. Johns Research Institute, India Makerere University, Uganda Kenya Medical Research Institute, Kenya Karolinska Institute, Sweden Wuhan University, China Albert Einstein College of Medicine, U.S. Arizona State University, U.S. Aurum Institute, South Africa Biomedical Primate Research Center, the Netherlands Case Western Reserve University, U.S. Centre for International Health, University of Bergen, Norway Colorado State University, U.S. Emory University, U.S. Food and Drug Administration, U.S. Foundation for Innovative New Diagnostics (FIND), Switzerland Harvard University, U.S. International AIDS Vaccine Initiative (IAVI), U.S. Johns Hopkins University, U.S. KNCV Tuberculosis Foundation, the Netherlands Leiden University Medical Center, the Netherlands Life Science Research Israel (LSRI), Israel Max Planck Institute for Infection Biology, Germany National Cancer Institute (NKI), the Netherlands Oregon Health Sciences University, U.S. Stanford University, U.S. Saint Louis University., U.S. Tuberculosis Vaccine Initiative (TBVI), Europe Tulane University, U.S. University of California-San Francisco, U.S. University of California-Los Angeles, U.S. University of Maryland, College Park, U.S. University of Tampere, Finland University of Wales, United Kingdom Vanderbilt University., U.S. Walter Reed Army Institute of Research, U.S. Foundations/ Governments/ NGOs Bill & Melinda Gates Foundation, U.S. Ministry of Foreign Affairs of Denmark The Netherlands Ministry of Foreign Affairs, the Netherlands Fogarty International Center and NIAID, National Institutes of Health, U.S. Research Council of Norway, Norway Maryland Department of Business and Economic Development, U.S. AIDS Fondet, Denmark Cambodian Health Committee, Cambodia European and Developing Countries Clinical Trials Partnership (EDCTP), European Commission LHL/ The Norwegian Association of Heart and Lung Patients, Norway Planeta Salud, Spain Mary Lynn Richardson Fund, U.S. Manhiça Health Research Centre, Mozambique Medicine in Need (MEND), U.S. Stop TB Partnership, Switzerland TB-Alert, United Kingdom Wellcome Trust, United Kingdom Foundations/Government/NGOs Academia Industry Industry GlaxoSmithKline Biologicals, Belgium Crucell, the Netherlands Statens Serum Institute, Denmark ImmunoBiology, United Kingdom Wuhan Institute of Biological Products, China Serum Institute, India Thymed, Germany Japan BCG Laboratory, Japan Korean Institute of TB, Korea Cyncron, Denmark Immune Solutions, New Zealand Sanofi Pasteur, France Smittskyddsinstitutet, Sweden Emergent BioSolutions, U.S. Intercell, Austria
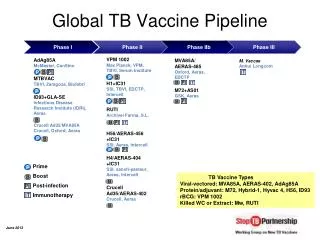
TB Vaccine Pipeline Additional research at the discovery/early pre-clinical level: Bhagawan Mahavir Medical Research Center; Cardiff University; EpiVax, Inc.; ImmunoBiology Ltd.; Infectious Disease Research Institute; Institute de Pharamacologie, Puso; Karolinska Institute; Malaysia-Finlay Institute, NIAID; NIH; Osaka University; Shanghai H&G Biotech; Sequella; UCLA; and, Vanderbilt University.
TB Vaccine Development Timeline Field Site Development ($2-4 million per yr, per site for 7 yrs) Costs associated with the development of all candidates in Aeras pipeline Challenge Models ($1 million per year for 7 yrs) Manufacturing ($5 million per yr for 9 yrs) Vaccine Discovery Pre-Clinical Testing Phase I Phase II Phase IIb Phase III Licensure 2.5 Years 2 Years 4 Years 1 - 2 Years 1 Year Costs related to the development of one TB vaccine candidate $160 Million $1.5 million $2.5 million $4 million $4 million • 4 of Aeras’ 6 TB vaccine candidates are in clinical trials in Africa; the others are expected to enter trials in 2010 • $160 million to conduct a Phase III licensure trial of one candidate • With sufficient resources, a new TB vaccine could be ready by 2016 • The Treatment Action Group estimated a $1.5 billion funding gap for TB research for 2008 alone
Recombinant BCG (rBCG) - A Better BCG • Safer in HIV infected infants or others with immune-suppression • BCG or rBCG boosted with another TB vaccine is much better than either vaccine alone • Constructed to over-express antigens from each stage of the TB life cycle • Prevent infection and reactivation utilizing “prime-boost” regimens • A new vaccine candidate with all of these properties is expected to enter clinical trials in 2010
Very small particles (2-4 microns) get deep into the lung, where infection occurs Aerosol delivery may provide an easy, affordable delivery mechanism that could eliminate the need for needles and cold chain and provide superior protection Aerosol Delivery of New TB Vaccines Spray Drying
Example of Site Development: South Africa • Partnership with South African Tuberculosis Vaccine Initiative (SATVI) • Field site developed in Worcester (~120 km from Cape Town) • Infrastructure developed: • State-of-the-art immunology laboratory • Highly skilled staff capable of performing the duties necessary to maintain the infrastructure and execute clinical research • Clinical and office facilities • Professional Development Program (Siyantinga- “Reach for the Stars”) – program initiated in 2001 • Resource Center established in 2005
Accomplishments in South Africa • South African Tuberculosis Vaccine Initiative - Most advanced site for large-scale TB vaccine trials in the world • BCG randomized clinical trial of 11,680 infants • Cohort studies involving more than 11,500 infants and adolescents • Conducting Phase I and Phase II studies of 4 vaccine candidates, first Phase IIb preliminary efficacy study of a new TB vaccine in infants in 80 years • 231 staff trained since 2004, including 162 female staff • Establishment of a Quality Management System and data capture mechanism
Capacity Building Highlights at Other Sites • State-of-the-art immunology and mycobacteriology lab developed in India - first of its kind in the area • State-of-the-art lab and case verification ward opened in Uganda • Quality management and data management infrastructure developed in India and Uganda • Professional Development Programs • Phase I trial at Kenya site • Planned multi-country Phase II trials
Benefits of Site Development and Clinical Research • Retain local talent and expertise • Raise awareness about TB in the community • Support and enhance local clinical research capacity • Community health and education • Infrastructure remains in the community • Leverage investment in infrastructure to use for clinical trials of other diseases
Vaccine Efficacy Trials MVA85A/AERAS-485 • First efficacy trial of a new TB vaccine in infants in more than 80 years • 2,800 infants • In collaboration with SATVI, Oxford-Emergent Tuberculosis Consortium and Wellcome Trust Additional Proof-of-Concept Studies Planned for 2010
Building manufacturing capacity and partnershipsnow to: Reduce the cost and time to manufacture and deliver vaccines to all who need them Produce enough bulk doses of vaccine to meet the world’s estimated need Work with partners in countries such as India, China, Korea and South Africa to produce, fill, finish and distribute vaccines at the lowest possible price Ensure uniformity of quality Minimize lag time between licensure and distribution Novel Approaches to Manufacturing
Access and Availability • Future access considered at every stage of vaccine development • Manufacturing • Guarantee by partners for sufficient production and affordable prices, or technology transfer • Manufactured by Aeras with partners in developing world • Aeras will not consider vaccine candidates that will be costly to manufacture on a large scale • Pricing • Dual pricing for affordable distribution in resource-poor countries • Cost plus purchase from partner • Aeras provides at cost • Distribution • Developing world governments • International organizations (GAVI, UNICEF) • Developing world partners
Aeras gratefully acknowledges the support of the following major donors THE MARY LYNN RICHARDSON FUND Netherlands Ministry of Foreign Affairs Ministry of Foreign Affairs of Denmark
Thank You! For more information: www.aeras.org pwillingham@aeras.org