Download
1 / 29
290 likes | 302 Views
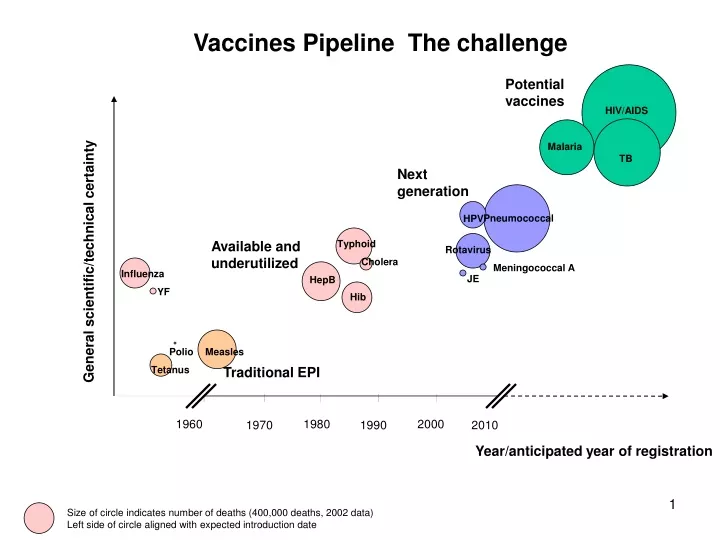
Hib. Vaccines Pipeline The challenge. Potential vaccines. HIV/AIDS. Malaria. TB. Next generation. Pneumococcal. HPV. Available and underutilized. Typhoid. Rotavirus. General scientific/technical certainty. Cholera. Meningococcal A. Influenza. JE. HepB. YF. Polio. Measles.

E N D
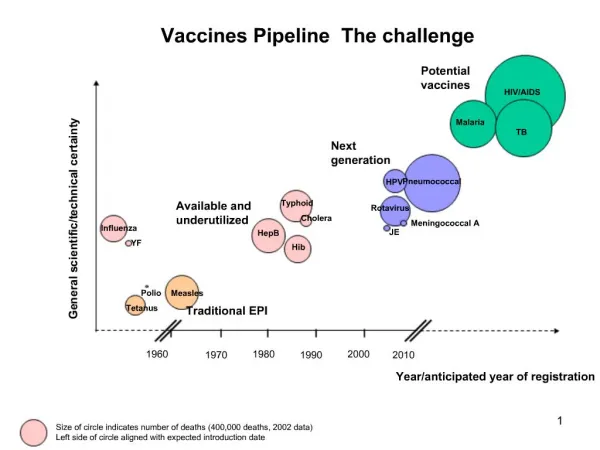
Hib Vaccines Pipeline The challenge Potential vaccines HIV/AIDS Malaria TB Next generation Pneumococcal HPV Available and underutilized Typhoid Rotavirus General scientific/technical certainty Cholera Meningococcal A Influenza JE HepB YF Polio Measles Tetanus Traditional EPI 1960 1980 2000 1970 1990 2010 Year/anticipated year of registration Size of circle indicates number of deaths (400,000 deaths, 2002 data) Left side of circle aligned with expected introduction date
7 million premature deaths from diseases for which vaccines are not yet widely available 3 million premature deaths from vaccine preventable diseases Hib Vaccines Pipeline The challenge HIV/AIDS Malaria TB Pneumococcal HPV Typhoid Rotavirus General scientific/technical certainty Cholera Meningococcal A Influenza JE HepB YF Polio Measles Tetanus 1960 1980 2000 1970 1990 2010 Year/anticipated year of registration Size of circle indicates number of deaths (400,000 deaths, 2002 data) Left side of circle aligned with expected introduction date
Developing a new vaccine takes 7-20 years – assuming success at each stage– and costs hundreds of millions dollars. Expectations of future market determines today’s investment decisions and, therefore, tomorrows products. 1 2 3 4 5 6 7 8 9 10 11 12 13 Product Development Cycle Low probability of market return Manufacturing capacity scale-up Decision gate: Probability of a market return? A disincentive to invest Efficacy trials (phase III) Cumulative investment Primate/ early clinical Research/pre-clinical ? 0 Elapsed time (years) Source: Mercer Management Consulting analysis
Slow introduction: Introduction of Hep B and Hib vaccines into developing countries is occurring 10-15 years after initial availability HepB -- all developing countries The Vaccine Fund established Hep B licensed in U.S. HepB -- all developing countries, excl. India, China, Indonesia Million doses Hib licensed in U.S. Hib -- all developing countries 1983 1985 1987 1989 1991 1993 1995 1997 1999 2001 2003 2005 GAVI forecasts*
Package of solutions • Buying and using existing products (GAVI, IFFIm) • Improves market for existing products • Strengthens delivery systems to reach children • Increases predictability of funding • Prepare for future products (GAVI, PPPs, WHO…) • Provide data for timely national decision on demand • Improve accuracy of forecasting • Invest public resources in early R&D • Product-development PPPs • “Enterprise” for scientific collaboration Missing: Assurance that the market for future products will exist
Vaccine for wealthy countries Vaccines for poor countries Health R&D for wealthy countries$106 billion Private investment to complete the pipeline Health R&D for poor countries$8 billion Funding the pipeline Discovery &Research Early Development Late Development CapacityInvestment Licensure Supply
Advance Market Commitments (AMC) Problem • Small, risky and unpredictable markets leads to under-investment in products of importance to the developing world • Industry’s investments in development/capacity determine what products are available, when and to whom Solution • Assurances of a future market as incentive for more timely investment by industry • Provide credible commitments to guarantee future financing for priority vaccines – before funds are needed to purchase doses • Only use funds – and buy vaccines - if there are results
Supply Price- Industrial Price – Middle Income Price – Low income Typical vaccine supply and pricing $ Price per dose Millions of doses 1 5 10 15 Years after licensure
AMC prices 12 10 Price GuaranteedAMC price 8 6 AMC $x billion Post-AMC market 4 2 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Years
AMCs: A market-based incentive • Create a market: for new vaccines needed in poor countries (not a purchase guarantee) • Donors commit upfront: Donors fund an AMC of a specified market size and price for a target vaccine with set specifications (effectiveness, public health impact) • Candidate vaccines become available: an Independent Assessment Committee determines if a vaccine meets the target specifications • Country demand: Where recipient countries are interested in introducing a successful candidate vaccine, donors subsidize its purchase and recipient countries provide co-payment. • Post-AMC predictable supply and pricing: When AMC funding is depleted, manufacturer continue to provide the vaccine at an established price for a specified period.
Market incentives… An AMC is tailored to the technical challenges and market conditions of each disease to provide an appropriate incentive for greater investment • Market entry: Open to all players – multinational and emerging, biotechs and vaccine manufacturers • Competition: Designed to sustain 2-3 firms to encourage adequate capacity and price competition • Continued innovation: Designed to last 7-10 years to allow time for 2nd and possibly 3rd generation products
The objective is to motivate increased investment and activity across the R&D pipeline, enabling the availability of better vaccines, sooner. Late-Stage: Continue/accelerate late development Increase planned manufacturing capacity In-Market: Increase capacity Early-Stage: Advance proof-of-concept Resurrect latent projects Research: Stimulatenew or refocus research activity Research Pre-Clinical Phase I Phase III Build capacity Approval In Market Phase II • HIV/AIDS • Malaria • TB • Pneumococcal • Rotavirus • HPV
Second Vaccine Approved First Vaccine Approved AMC Commitment exhausted Framework AgreementAnnounced • Suppliers provide vaccine to eligible countries at agreed lower price Guarantee Agreement 1 • Price guarantee • Manufacturing capacity • Vaccines delivered Guarantee Agreement 2 Details on AMC: Size, price, target product goal • Second vaccine purchased Legal framework Framework Agreement • Donors sign binding financial commitments • Companies sign on
AMC complements other strategies • Increased investment in R&D (push) • Direct investment in vaccine candidates • Investment in establishing development capacity (clinical trial field sites etc) • Investment in public-private partnerships • Strengthened delivery systems to ensure vaccines reach target populations • Strengthened demand forecasting to reduce industry risk • Strengthened national planning of health priorities and budgets • Credible assurance of future commitment to purchase priority new vaccines -- AMC
Next steps • Technical dialogue on AMC as requested • Further work on ….. • Second meeting of Donor Consortium in late-October
AMC IFFIm: frontloaded, predictable resources Annual pledges $ to subsidize country co-pay for specified vaccine $ $ GAVI Support for 72 poorest countries (vaccines, funds for systems, TA) GAVI, IFFIm and AMCs … TNZ CAR Ken Nig Eth Laos Cam Haiti Tajik
“Typical” vaccine pricing Gradual Market penetration New on market Mature product Year from first licensure 1-5 years Capacity small, few suppliers (usually 1 or 2) Prices premium Limited to wealthiest 6-10 years Capacity expanding with experience, 2 -3 suppliers Prices tier for industrial and middle income Industrial plus middle income countries 10-15+ High capacity Better yields and 3-6 suppliers Prices lower, tiered for industrial, middle income low income countries Global Capacity Pricing Availability
The case for vaccines • Safe, effective, sustainable • Low systems costs • Highly cost effective • $15-30 per DALY • $100 yardstick in developing countries • $100 000 yardstick in US • Huge benefits • Lives saved • Economic productivity • Demographic transition • 50% improved standard of living in 20th Cthe result of improved longevity References: See Barder, Kremer, Williams (2006)
Advance Market Commitments Response to Vaccine and Biotech Industry’s concerns to initial AMC proposal
Size of the AMC • CGD proposal: $3.0 billion AMC size for all products (average market size for successful pharmaceutical products • Industry reaction: Market size most critical factor in AMC. Size must be tailored to specific scientific and market conditions • Current AMC work: AMC estimates tailored to each product based on risk-adjusted, net-present value return to industry. Model allows scenarios to be run with different assumptions.
Continuing Demand Uncertain • CGD proposal: The proposal assumed that the AMC guarantee addresses financing risk and demand risk • Industry reaction: There is a continued high level of risk associated with timely knowledge about developing country demand for vaccines even with AMC support. • Current AMC work: Agree, ongoing discussion to explore parallel activities to improve accuracy of forecasts e.g. • support PPPs and other partners in ensuring gov’ts have necessary data to make decisions • Strengthen forecasting • Explore gov’ts signing intent to introduce or not to introduce an AMC vaccine • Explore possibilities of capital investment or small guarantees through other entities
Post-AMC pricing and volume commitments • CGD proposal: Once AMC depleted, companies benefiting from the AMC would be required to drop prices substantially (marginal costs discussed) and commit to supply to meet all demand from eligible developing countries • Industry reaction: Commiting to a long-term (post-AMC), low prices before there is knowledge about the costs of production or investment might mean companies forced to sell at a loss. No company will commit to this. • Current AMC work: Agree, ongoing discussion to explore options. • Favored idea is that each firm sets post-AMC price at time that they submit product for review to the IAC. Post-AMC price then used to establish co-pay so incentive for industry to keep low.
Superiority vs Comparability for Second Entrants • CGD proposal: The second entrant to the AMC would be required to prove their product was superior to the first entrant • Industry reaction: Extremely complex to implement • Current AMC work: Agree, this is now deleted from the AMC. Any products that meet the IAC product standards are eligible for AMC funding. Multiple entrants will be encouraged (through decisions on size and duration of AMC) to assure capacity and promote competition.
Structure and Function of the IAC • CGD proposal: An independent expert body needed to set the product Goals to trigger an AMC and determine if a given product achieves the goal. Also need entity to lower requirements in necessitated. • Industry reaction: Unease over adding another layer of bureacracy on-top of national licensing requirements and WHO pre-qualification • Current AMC work: Understand concern but IAC plays unique role. Attempt to minimize requirements and avoid any duplication • Endorse licensing decision of credible NRA • Set public health performance goal for target countries • Early communication of minimum data to show performance • Working with WHO to harmonize with pre-qualification process
Credibility of donor agreements • CGD proposal: Guarantee agreement with each qualifying firm is signed by all donor governments with donors making binding commitments. • Industry reaction: Transaction costs and risk of donor reneging too high with multiple signatories or multiple contracts. • Current AMC work: Agree, donors also wish to avoid complexity of multiple signatories and multiple contracts. On-going discussion to explore options but probable that a single agent for the donors will hold binding commitments and sign contracts on strength of commitments.
Product Specifications • CGD proposal: IAC should define the product goals that will trigger AMC funding. • Industry reaction: Value in having clear product goal but the actual product specifications will strongly affect the attractiveness of the AMC. • Current AMC work: Understood. Work on-going to determine AMC composition to ensure critical skills and knowledge on public health goals, state of science and commercial implications product goals. Uncertain how to engage firms without losing independence and credibility of decision.
Milestone payments or push funding • CGD proposal: AMCs are a market based mechanism that ensures funding at a reasonable price when the desired product is demanded by a given government. • Industry reaction: The market return is far in the future for early stage and still has large demand risks. Milestone payments at key points (e.g. proof of concept, finish 2b clinical trial, finish phase 3 trials, make capital investment in capacity) • Current AMC work: Understand but not feasible within the AMC given G8 focus on market mechanism. Flat payments to industry too risky and politically untenable. Will explore potential of other partners to make investment with link back to AMC.
AMCs: A market-based incentive AMCs are designed to provide an adequate return on manufacturer investment in target vaccines. AMC process: • Donors commit to fund AMC for target vaccine. • Target vaccine specifications (effectiveness, public health impact), tailored AMC market size and AMC price are established. • An Independent Assessment Committee determines if a vaccine meets the target specifications. • When a vaccine meets the specifications and countries are interested in introducing the vaccine, donors pay subsidy and recipient countries provide co-payment. • When AMC funding is depleted, manufacturer is obligated to continue to provide the vaccine at an established price for a specified period. AMC complements direct R&D funding as well as efforts to strengthen current immunization programs and systems.