Download
1 / 42
420 likes | 566 Views
ACS CAN Legislative Priorities. A Primer on our Issues September 22, 2008. Who We Are & Why We Are Here. CATHY CALLAWAY - ACS CAN Senior Specialist, State And Local Campaigns GREGG HAIFLEY - ACS CAN Associate Director, Federal Relations

E N D
ACS CAN Legislative Priorities A Primer on our Issues September 22, 2008
Who We Are & Why We Are Here • CATHY CALLAWAY - ACS CAN Senior Specialist, State And Local CampaignsGREGG HAIFLEY - ACS CAN Associate Director, Federal Relations • WHY WE ARE HERE: To provide information on the ACS CAN State and Federal Legislative priorities to empower advocates to secure passage of legislation to prevent, screen for, and treat cancer.
Who We Are & Why We Are Here • JOHN DANIEL - South Atlantic Division, Vice President, Federal & Emerging Issues • PETER AMES – New England Division, State Director of Government Relations & Advocacy • WHY WE ARE HERE: To provide information on the ACS CAN State and Federal Legislative priorities to empower advocates to secure passage of legislation to prevent, screen for, and treat cancer.
State Issues • Colorectal Cancer Screening • Pain & Palliative Care • Breast & Cervical Cancer Screening • Tobacco Control
Colorectal Cancer Screening ACS & ACS CAN believe all patients, in consultation with their doctor, should have access to the full range of colorectal cancer screening tests that are best for that individual's medical situation, and that all screening tests should be covered by private insurance for employees of all size companies regardless.
Colorectal Cancer Screening • This year, the American Cancer Society, in conjunction with many other professional medical organizations, released new, updated screening guidelines for colorectal cancer. • 26 states and the District of Columbia now have cancer screening mandates in effect for private insurance. • Many states have begun programs to screen for and treat colorectal cancer in uninsured populations.
Access to Care-Colorectal Cancer Screening Coverage WASHINGTON 2007 VERMONT 2006 MAINE 2008 NORTH DAKOTA • FLORIDA MONTANA MINNESOTA 2007 OREGON 2005 NEW HAMPSHIRE IDAHO WISCONSIN SOUTH DAKOTA MASSACHUSETTS NEW YORK** 2004 WYOMING 2001 MICHIGAN RHODE ISLAND 2000 CONNECTICUT 2001 IOWA PENNSYLVANIA NEBRASKA 2007 NEW JERSEY 2001 NEVADA 2003 OHIO DELAWARE 2000 UTAH INDIANA 2000 ILLINOIS 2003* * WEST VIRGINIA 2000 MARYLAND 2001 COLORADO VIRGINIA 2000 CALIFORNIA 2000 KANSAS MISSOURI 1999 DISTRICT OF COLUMBIA 2002 KENTUCKY 2008 NORTH CAROLINA 2001 TENNESSEE ARIZONA OKLAHOMA SOUTH CAROLINA NEW MEXICO 2007 ARKANSAS 2005 GEORGIA 2002 MISSISSIPPI ALASKA 2006 ALABAMA TEXAS 2001 LOUISIANA 2005 HAWAII Screening law ensures coverage for the full range of tests Screening law requires insurers to cover some tests, but not the full range or Statewide insurer agreements are in place to cover the full range of tests Screening law requires insurers to offer coverage, but does not ensure coverage or There are no state requirements for coverage Sources: Health PolicyTracking Service & Individual state bill tracking services *In 2003, Illinois expanded its 1998 law to cover the full range **The New York Health Plan Association, which serves 6 million New Yorkers, covers the full range of colorectal cancer screening tests, as a part of a voluntary collaborative with ACS.
Pain and Palliative Care ACS & ACS CAN believe that the full range of cancer pain relief treatments and medications should be available to all cancer patients and that approved and legal cancer pain relief medications should be attainable without undue scrutiny or suspicion cast upon the cancer patient who may rely on those medications for medical and/or quality of life purposes.
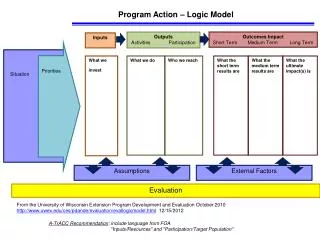
Pain and Palliative Care • 31 states have a ‘B’ or better on the University of Wisconsin's Pain & Policy Studies Group (PPSG) report card. • 5 states have achieved an ‘A’ • In September, new model legislation and policy guidelines regarding state electronic prescription monitoring programs (PMPs) were rolled out to the field.
Cancer Pain Management: 2008 State Policies and Practice WASHINGTON FLORIDA VERMONT MAINE NORTH DAKOTA MONTANA MINNESOTA OREGON NEW HAMPSHIRE IDAHO WISCONSIN SOUTH DAKOTA MASSACHUSETTS NEW YORK MICHIGAN WYOMING RHODE ISLAND CONNECTICUT PENNSYLVANIA IOWA NEBRASKA NEVADA OHIO NEW JERSEY UTAH INDIANA ILLINOIS DELAWARE * WEST VIRGINIA MARYLAND COLORADO WASHINGTON, D.C. VIRGINIA CALIFORNIA KANSAS MISSOURI KENTUCKY NORTH CAROLINA TENNESSEE OKLAHOMA ARIZONA SOUTH CAROLINA ARKANSAS NEW MEXICO ALASKA GEORGIA MISSISSIPPI ALABAMA Well balanced policies and good practices that enhance pain management, with opportunities for additional improvements to achieve better pain management TEXAS HAWAII LOUISIANA Moderately balanced policies and practices; action required to address some policy and practice barriers that impede pain management *Source: Data from University of Wisconsin’s Pain & Policy Studies Group, Achieving Balance in State Pain Policy: A Progress Report Card (2008). http://www.painpolicy.wisc.edu/Achieving_Balance/index.html Numerous policy and practice barriers exist that impede pain management and require concerted action to address
State Appropriations for Breast & Cervical Cancer Screening Programs WASHINGTON • FLORIDA VERMONT NORTH DAKOTA MAINE MONTANA MINNESOTA OREGON NEW HAMPSHIRE IDAHO WISCONSIN SOUTH DAKOTA MASSACHUSETTS NEW YORK WYOMING MICHIGAN RHODE ISLAND CONNECTICUT IOWA PENNSYLVANIA NEBRASKA NEW JERSEY NEVADA OHIO DELAWARE UTAH INDIANA ILLINOIS* * WEST VIRGINIA MARYLAND COLORADO VIRGINIA CALIFORNIA KANSAS MISSOURI DISTRICT OF COLUMBIA KENTUCKY NORTH CAROLINA TENNESSEE ALASKA ARIZONA OKLAHOMA SOUTH CAROLINA NEW MEXICO ARKANSAS GEORGIA MISSISSIPPI ALABAMA American Cancer Society National Government Relations Department Policy Updated June 20, 2008 TEXAS LOUISIANA HAWAII State Allocation/CDC award > 100.0% States do not allocate funding more than the required match State Allocation/CDC award between 0.01-99.9% Source: 2007 data from the Centers for Disease Control and Prevention and unpublished data collected from NGRD, Divisions, including input form NBCCEDP directors. * Illinois expanded their program to serve all uninsured women in Illinois in the age group served.
Policy Initiatives to Fight Breast & Cervical Cancer • Protect the Breast and Cervical Cancer Prevention and Treatment Act • Funding the Patient Navigation Program • Eliminate Medicare co-pays for breast screening services • Increase access, education and use of the HPV vaccine. • Ensure quality healthcare is available to all.
Tobacco Control • Smoking accounts for at least 30% of all cancer deaths and 87% of lung cancer deaths. • The Solution: • Regular increases in the price of tobacco products • Fully funding & implementing comprehensive research-based tobacco control programs according to CDC’s Best Practices • Passing & implementing smoke-free policies
State Cigarette Tax Rates WASHINGTON $2.025 FLORIDA VERMONT $1.99 MAINE NORTH DAKOTA $2.00 MONTANA MINNESOTA $1.70 44¢ $1.504 OREGON NEW HAMPSHIRE $1.08 $1.18 IDAHO WISCONSIN SOUTH DAKOTA 57¢ $1.77 $2.75 MASSACHUSETTS $2.51 $1.53 NEW YORK MICHIGAN WYOMING $2.00 RHODE ISLAND $2.46 60¢ CONNECTICUT $2.00 PENNSYLVANIA IOWA $1.36 $1.35 NEBRASKA NEVADA 64¢ OHIO NEW JERSEY $2.575 80¢ $1.25 UTAH INDIANA DELAWARE $1.15 ILLINOIS 69.5¢ 98¢ 99.5¢ WEST VIRGINIA * MARYLAND $2.00 COLORADO 55¢ WASHINGTON, D.C. $1.00 84¢ VIRGINIA CALIFORNIA KANSAS 30¢ 30¢ MISSOURI 87¢ 79¢ 17¢ KENTUCKY NORTH CAROLINA 35¢ TENNESSEE 62¢ OKLAHOMA ARIZONA SOUTH CAROLINA $2.00 $1.03 ARKANSAS NEW MEXICO ALASKA 91¢ 59¢ $2.00 7¢ GEORGIA MISSISSIPPI 18¢ 37¢ ALABAMA 42.5¢ 36¢ TEXAS $1.41 LOUISIANA 33.9¢ HAWAII $1.80 Equal to or above $1.14 per pack Between $0.57 and $1.13 per pack Equal to or below $0.56 per pack
Tobacco Control Funding • ACS & ACS CAN support funding and implementation of tobacco control programs according to the 2007 CDC Best Practices for Comprehensive Tobacco Control Programs • State & Community Interventions • Health Communications Interventions • Cessation Interventions • Surveillance & Evaluation • Administration & Management
100% Smoke-free Policies • 65.1% of US population protected by 100% smoke-free workplace and/or restaurant and/or bar law. • 2,883 municipalities restrict smoking • 28 states plus DC & Puerto Rico have strong smoke-free laws
Percent of US Population Protected • 49.7% of US population resides in a community with a smoke-free workplace law. • 62.6% with a smoke-free restaurant law • 50.6% with smoke-free bar law • 34.7% have 100% smoke-free workplaces & restaurants & bars.
FEDERAL ISSUES • GRANTING FDA THE AUTHORITY TO REGULATE THE PRODUCTION AND MARKETING OF TOBACCO PRODUCTS
FEDERAL ISSUES • INCREASING FUNDING FOR RESEARCH FOR CANCER PREVENTION AND EARLY DETECTION, AND TREATMENT
FEDERAL ISSUES • ESTABLISH A CDC COLORECTAL CANCER SCREENING AND TREATMENT PROGRAM AND INCREASE FUNDING OF THE CDC NATIONAL BREAST AND CERVICAL CANCER EARLY DETECTION PROGRAM (NBCCEDP)
FDA REGULATION OF PRODUCTION AND MARKETING OF TOBACCO PRODUCTS HR 1108/S 625 • Stops aggressive tobacco company marketing to children – curbs youth access to tobacco products • Requires unmistakable health warnings on packages • Requires tobacco companies to disclose the content of their products
FDA REGULATION OF PRODUCTION AND MARKETING OF TOBACCO PRODUCTS HR 1108/S 625 • Allows FDA to order changes in tobacco products. • Stops the tobacco industry from making false and misleading claims about their products. • Gives states and local governments authority to regulate tobacco marketing within their jurisdictions.
WHAT THE FDA BILL DOES NOT DO • Does not overtax the resources and capability of the FDA • Does not mislead the public into thinking that the FDA has found tobacco products to be safe to consume • Does not assert any new authority over tobacco farms or tobacco growers • Does not add to the annual federal deficit or to the national debt
THE BUDGET AND THE NATIONAL CANCER FUND • Cancer research and prevention funding has not kept pace with inflation and increased needs. • Since FY 2003, when accounting for inflation, the NCI’s budget has decreased by more than $630 million (13.7 percent). • Since FY 2003, CDC’s cancer budget has shrunk by nearly $14 million (5 percent) • In FY 2007, NCI funded 300 fewer new research project grants than just three years ago.
WHY FUNDING MUST INCREASE • Research is providing breakthroughs in prevention and early detection, and new treatments for the deadliest cancers. • But the budgets for NCI and CDC cancer programs are falling below where they need to be. • Fewer clinical trials have been started and fewer patients are being enrolled than five years ago.
WHY FUNDING MUST INCREASE • The development of new drugs, devices, and other tools for treating cancer is being delayed. • CDC’s National Breast and Cervical Cancer Early Detection Program served 44,000 fewer women in 2006 than in 2005 – a decline of 7.5 percent. • CDC’s colorectal cancer screening initiative is under-funded and unable to increase public awareness about the need for colorectal screening. Full funding of the national colorectal screening and treatment program would cost approximately $525 million a year and would save more than 30,00 lives.
THE FUNDING WE NEED – FY 2009 • National Institutes of Health - $30.81 billion ($1.88 billion (6.5 percent) over FY 2008) • National Cancer Institute - $5.26 billion ($455 million (9.5 percent) over FY 2008) • Centers for Disease Control Cancer Programs - ($136 million over FY 2008)
WE WON’T ACCEPT EXCUSES • Appropriations bills aren’t going anywhere this year …. • Response: The funding bills will have to be passed at some point (early next year if not late this year) – will you support our funding increase request?
WE WON’T ACCEPT EXCUSES • We just doubled NIH’s budget …. • Response: If you take inflation into account, the funding is down
WE WON’T ACCEPT EXCUSES • NIH needs to do a better job managing its money …. • Response: Nearly 80 percent of the NCI portion of NIH funding goes out the door to support research at more than 650 universities, hospitals, cancer centers, and other sites across the country. Research leads to breakthroughs in screening and treatments and often leads to clinical trials that directly benefit cancer patients.
WE WON’T ACCEPT EXCUSES • Wasn’t there just a big fundraiser for cancer? • Response: Stand Up To Cancer generated about $100 million in pledged donations for cancer research – a good thing but not enough to meet our research needs.
THE NATIONAL CANCER FUND - HR 6791 • Provide a dedicated source of funding to supplement existing appropriations of funds for combating cancer. • Increased, sustainable and predictable funding would allow for long-term planning and support for cancer research, early detection, and screening projects. • Dedicated, sensible, sustainable, well supported funding.
BENEFITS OF A NATIONAL CANCER FUND • Expanded access to health care for underserved and underinsured. • New research to discover prevention and early detection tools for the most deadly cancers, including, but not limited to, pancreatic, ovarian, and lung cancers.
BENEFITS OF A NATIONAL CANCER FUND • Expanded breast and cervical cancer early detection and treatment programs to cover screening and treatment for women who do not have access to health care. • Expanded colorectal cancer early detection and treatment programs to cover men and women who do not otherwise have access to health care.
BENEFITS OF A NATIONAL CANCER FUND • Increased number of qualified NIH research grants. • Increased access to federally sponsored clinical trials.
ESTABLISH A CDC COLORECTAL CANCER SCREENING AND TREATMENT PROGRAM • Colorectal cancer is the second most common cause of cancer death in men and women in the United States. • Yet, colorectal cancer can be prevented in many cases through the early identification and removal of pre-cancerous polyps, detectable only through colorectal cancer screenings.
ESTABLISH A CDC COLORECTAL CANCER SCREENING AND TREATMENT PROGRAM • Of the 49,960 people expected to die of colorectal cancer in 2008, 50-80% could be saved if they were tested. • The uninsured and underinsured are at particular risk of being diagnosed with later-stage colorectal cancer. Over 80 percent of uninsured adults between the ages of 50 and 64 have not been screened for colorectal cancer.
ESTABLISH A CDC COLORECTAL CANCER SCREENING AND TREATMENT PROGRAM • H.R. 1738 establishes a program at the CDC to provide screenings and treatment for colorectal cancer for low-income, uninsured and underinsured. • The Senate Labor/HHS appropriations bill includes $25 million for CDC to spend through pilot sites to do colorectal cancer screening – this would allow CDC to expand its current colorectal cancer screening efforts.
INCREASE FUNDING OF NATIONAL BREAST AND CERVICAL CANCER EARLY DETECTION PROGRAM (NBCCEDP) • The NBCCEDP provides low-income, uninsured and underinsured women access to breast and cervical cancer screening tests, follow-up services and access to treatment. • Since its inception in 1991, the NBCCEDP has provided more than 7.5 million screening tests to more than 3.1 million women and diagnosed more than 33,000 breast cancers, 2,000 cervical cancers and 88,000 pre-cancerous cervical lesions.
INCREASE FUNDING OF NATIONAL BREAST AND CERVICAL CANCER EARLY DETECTION PROGRAM (NBCCEDP) • However, NBCCEDP served 44,000 fewer women in 2006 than in 2005 – a decline of 7.5 percent. • Fulfill the promise of the NBCCEDP Reauthorization Act of 2007 by accelerating an increase in resources for the program to $250 million, which would allow at least an additional 130,000 women to be served.
Thank you! • Thank you for your advocacy. • Together we will make a difference. • Success will mean reducing the incidence of cancer, increasing screening, expanding research, securing treatment, and saving lives.