Download
1 / 15
150 likes | 310 Views
Clarifying Key Concepts. Objective. To clarify key concepts that a majority did not know the answer for on the knowledge test taken at the end of the training The components of an effective team structure Designated and situational leaders

E N D
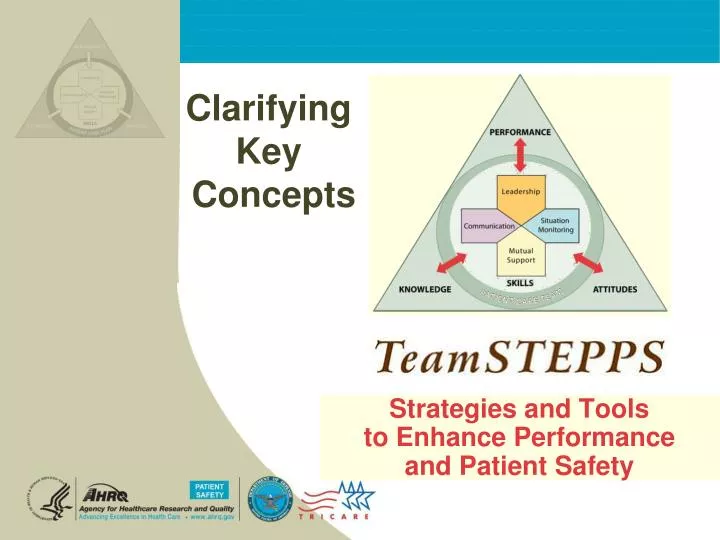
Clarifying Key Concepts
Objective • To clarify key concepts that a majority did not know the answer for on the knowledge test taken at the end of the training • The components of an effective team structure • Designated and situational leaders • The role of a structured framework in information exchange • What makes handoffs different from other communication? • What is a shared mental model? • What is mutual support?
TeamSTEPPS is composed of four teachable/learnable skills • Leadership • Situation Monitoring • Mutual Support • Communication • Skills are supported by team structure …team performance is a science…consequences of errors are great…
Components of Effective Team Structure • A team is composed of two or more people who… • Interact interdependently and adaptively • Have complementary skills • Have effective leadership • Work toward a common goal… this is the MOST important component of team structure…knowledge of the common goal accounted for 14% of the difference in team function • Have clear roles and responsibilities…second most important component of team structure…accounted for 12% of the difference in team function • Hold them selves mutually accountable for achieving the goal Salas et al. Does team training work? Principles for health care. AcadEmerg Med. 2008. 15:1-8.
Designated and Situational Leaders • Leadership is one of the four key teachable/learnable TeamSTEPPS strategies • There are two type of leaders • Designated leader is assigned to lead and organize a designated core team by • Establishing clear goals • Facilitating open communication, information, and mutual support sharing through briefs, huddles, debriefs • Resolving conflict • Situational leader is any team member who steps forward because they have the skills/knowledge to manage the situation-at-hand; situational leader may step forward during a brief or debrief or they may call a huddle
Information Exchange Communication contributes to nearly 2/3 of sentinel events because effective communication does not come naturally http://www.jointcommission.org/assets/1/18/Root_Causes_Event_Type_04_4Q2012.pdf
Information Exchange • Effective communication is the exchange of information between a sender and a receiver…and it is • Complete • Brief • Clear • Timely • Closed loop by asking for confirmation and providing time for follow up questions • Structured communication strategies such as SBAR, Call-Out, Check-Back, and Handoffs decrease errors by setting expectation for what will be communicated
What makes Handoffs Different? • A handoff involves the transfer of information—along with authority and responsibility—during transitions in care across the continuum; • Because authority and responsibility are being transferred, the handoff must include opportunity to address • Safetyconcerns • Background…what are the co-morbidities, medications, history • Actions…what has already been done? • Timing…how urgent, what should be done first: • Ownership…who is responsible for what? • Next…what will happen next? • Which is why SBAR may not be the best tool for a handoff across shifts or levels of care unless it is modified
“I PASS THE BATON” Introduction: Introduce yourself and your role/job (include patient) Patient: Identifiers, age, sex, location Assessment: Present chief complaint, vital signs, symptoms, and diagnosis Situation: Current status/circumstances, including code status, level of uncertainty, recent changes, and response to treatment Safety: Critical lab values/reports, socio-economic factors, allergies, and alerts (falls, isolation, etc.) THE Background: Co-morbidities, previous episodes, current medications, and family history Actions: What actions were taken or are required? Provide brief rationale Timing: Level of urgency and explicit timing and prioritization of actions Ownership: Who is responsible (nurse/doctor/team)? Include patient/family responsibilities Next: What will happen next? Anticipated changes? What is the plan? Are there contingency plans? Question, Clarify, and Confirm
What is a Shared Mental Model? • A shared mental model is the perception of, understanding of, or knowledge about a situation or process that is shared among team members through communication • Shared mental models require individuals to monitor what is going on around them and share that information during briefs, huddles, and debriefs SituationMonitoring(Individual Skill) SituationAwareness(Individual Outcome) Shared Mental Model(Team Outcome)
What is a Mutual Support? • Mutual support is one of the four key skills or team strategies taught in TeamSTEPPS; the other three are leadership, situation monitoring and communication • Mutual support is “back up behavior” in which team members provide a safety net for each other to prevent errors Feedback focuses on behaviors and is needed to improve team performance Task Assistance can prevent work overload Patient Safety I’m Concerned, I’m Uncomfortable, this is a Safety issue! I must advocate for my patient; others may not have the same information
What is a Mutual Support? • Mutual support has the most tools of the four key strategies • Task assistance • Feedback • Advocacy and Assertion • Two Challenge Rule • CUS (resolve information conflict) • DESC Script (resolve personal conflict) • Advocating for patients may lead to conflict when decision makers don’t have the same information (shared mental model) or there is a personality conflict • Assertion is NOT aggressive; it does not undermine authority, attack the decision maker, or question a decision without reason Information Conflict Personal Conflict
Summary Teams provide organizations with a greater ability to adapt and learn than do individuals. However, just because groups of people call themselves a team doesn’t mean that they are truly a team. Based on an extensive review of the literature, Eduardo Salas and colleagues published the theoretical model on the next slide in 2005. This framework is called the big 5 of teamwork. The purpose of the model is to identify the core concepts that enable groups of people to work together, to collaborate, to adapt to changing circumstances, and effectively work toward a common goal. The diagram illustrates that when team leaders direct and coordinate the activities of other team members by clarifying roles, establishing goals & expectations, and organizing meetings for planning and feedback, they provide the opportunity for team members to communicate, collaborate, and cooperate. It is during these meetings—briefs, huddles, and debrief—that team members communicate what they have learned by monitoring others, a new shared mental model of how to reach a goal emerges, and team members offer back up or mutual support to achieve that goal. When team members trust each other, value team goals above individual goals, and use closed loop communication, they have the ability to be adapt, manage complex systems and complex patients and learn from experience.
Mutual Performance Monitoring The Theory Team Leadership Team Orientation Back-up Behavior Shared Mental Models Mutual Trust Adaptability Team Effectiveness Big 5 Salas, Sims, Burke. Is there a “Big Five” in teamwork? Small Group Research. 2005; 36:555-599. Coord. Mechanism Closed Loop Communication
Summary • Impact of errors…patients are harmed, non-clinical teams do not achieve goals • TeamSTEPPS Framework • Safety net for fallible human beings • TeamSTEPPS training meets a need • Diffuse evidence-based training program nationally and internationally http://teamstepps.ahrq.gov/ • Outcomes of TeamSTEPPS Shared Mental Model Adaptability Team Orientation Mutual Trust Team Performance Patient Safety!!