Download
1 / 24
240 likes | 658 Views
Autoimmune Hepatitis. Jeff Kiker and Amanda Daeges. What is autoimmune hepatitis?.

E N D
Autoimmune Hepatitis Jeff Kiker and Amanda Daeges
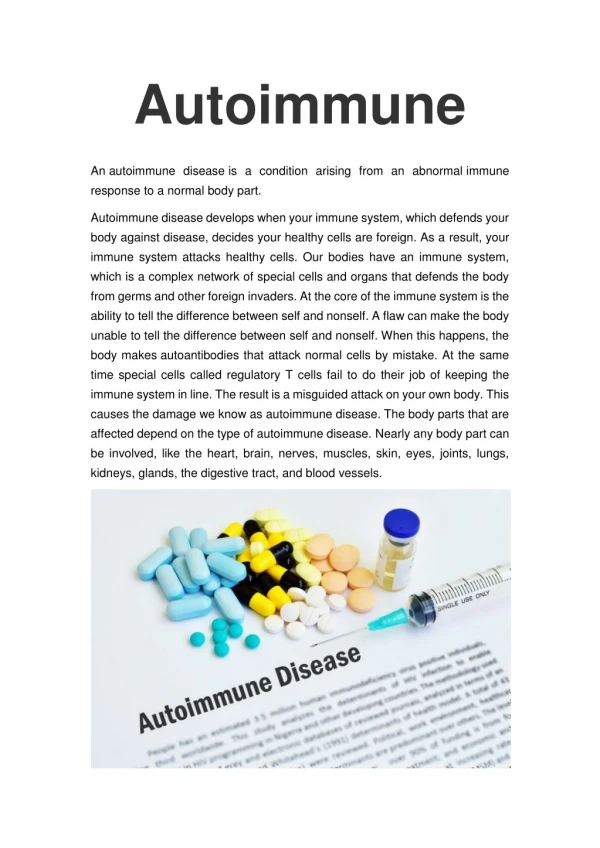
What is autoimmune hepatitis? • Autoimmune hepatitis is a disease in which the body’s own immune system attacks the liver and causes it to become inflamed. The disease is chronic, meaning it lasts many years. If untreated, it can lead to cirrhosis and liver failure. • There are two forms of this disease. Type 1, or classic, autoimmune hepatitis is the more common form. This is the form that mostly affects young women and is often associated with other autoimmune diseases. • Type 2 autoimmune hepatitis is less common and generally affects girls between the ages of 2 and 14. .
What causes autoimmune hepatitis? • Your immune system normally attacks bacteria, viruses and other invading organisms. It is not supposed to attack your own cells; if it does, the response is called autoimmunity. • In autoimmune hepatitis, your immune system attacks your liver cells, causing long-term inflammation and liver damage. • Scientists don’t know why the body attacks itself in this way, although heredity and prior infections may play a role.
What are the symptoms and complications of autoimmune hepatitis? Often, the symptoms of autoimmune hepatitis are minor. When symptoms do occur, the most common are • fatigue • abdominal discomfort • aching joints • Itching • jaundice • enlarged liver • nausea
Other symptoms may include dark urine, loss of appetite, pale stools and absence of menstruation. • More severe complications can include ascites (fluid in the abdomen) and mental confusion. • spider angiomas (blood vessels) on the skin. • In 10%-20% of cases, autoimmune hepatitis may present with symptoms like an acute hepatitis.
How is autoimmune hepatitis diagnosed? • Autoimmune hepatitis often occurs suddenly. Initially, you may feel like you have a mild case of the flu. As PE does not often offer the examiner much information to confirm a diagnosis of autoimmune hepatitis, your doctor will need to use…blood tests and a liver biopsy • antinuclear antibody (ANA), • smooth muscle antibody (SMA), • Liver/kidney microsomal antibody (LKM-1) • and anti-mitochondrial antibody (AMA) • are all of use, as is finding an increased Immunoglobulin G level. • However, the diagnosis of autoimmune hepatitis always requires a liver biopsy. • In complex cases a scoring system can be used to help determine if a patient has autoimmune hepatitis, which combines clinical and laboratory features of a given case.
Liver biopsy histology at initial presentation showing peri-portal lymphocytic infiltration and extensive peri-portal fibrosis.
Four subtypes are recognized, but the clinical utility of distinguishing subtypes is limited. • Positive ANA and SMA, raised immunoglobulin G (classic form, responds well to low dose steroids) • Positive LKM-1 (typically female children and teenagers; disease can be severe) • All antibodies negative, positive antibodies against soluble liver antigen (SLA)(now designated SLP/LP). This group behaves like group 1. • No autoantibodies detected (~13%)
Who is at risk for autoimmune hepatitis? • About 70 percent of people with autoimmune hepatitis are women, usually between the ages of 15 and 40. • Many people with this disease also have other autoimmune diseases, including type 1 diabetes, thyroiditis (inflammation of the thyroid gland), ulcerative colitis (inflammation of the colon), vitiligo (patchy loss of skin pigmentation), or Sjogren’s syndrome (dry eyes and dry mouth)
How is autoimmune hepatitis treated? • The goal of treatment is to stop the body’s attack on itself by suppressing the immune system. • prednisone,, • azathioprine (Imuran) • Treatment starts with a high dose of prednisone. When symptoms improve, the dosage is lowered and azathioprine may be added.In most cases, autoimmune hepatitis can be controlled but not cured. That is why most patients will need to stay on the medicine for years, and sometimes for life. • long-term use of steroid can cause serious side effects including diabetes, osteoporosis, high blood pressure, glaucoma, weight gain and decreased resistance to infection.
Black Cohosh causes AI Hep • The mechanism of action of black cohosh remains unclear, and the effects on estrogen receptors or hormonal levels, if any, have not been fully elucidated. Safety and efficacy data beyond six months are not available," she added. • Dr. Cohen and colleagues came to the conclusion that their patient, a 57-year old woman, likely suffered from black cohosh–induced autoimmune hepatitis after exhaustive examination. • The woman, who presented with history of increasing fatigue and lethargy for two weeks, was receiving treatment for diabetes mellitus and hypertension, he said. • For at least two years, she had been taking labetolol, fosinopril, verapamil, metformin, aspirin, and insulin. • At the advice of her primary physician, she had recently stopped HRT. She had started taking black cohosh three weeks prior to the onset of symptoms.
Black Cohosh causes AI Hep • The patient said she did not drink, smoke, or use intravenous drugs, and had had no transfusions, tattoos, or recent travel to areas in which hepatitis is endemic. • Physical examination was unrevealing, Dr. Cohen said. Hepatitis A, B, and C serologies and smooth muscle antibodies were negative, but alkaline phosphatase was mildly elevated and antinuclear antibodies were positive at 1:640. • A liver biopsy revealed piecemeal necrosis and lobular infiltrates with extensive plasma cells and eosinophils, both features of autoimmune and drug-induced hepatitis, Dr. Cohen said. • Black cohosh was discontinued, and the woman's symptoms resolved completely after two weeks. A tapering course of prednisone was started, Dr. Cohen said, and liver function tests were back to normal about nine weeks later.
Did Black Cohosh cause an CYP enzyme shift? Or was it secondary to d/c HRT • Reports of liver injury have been cited for • Labetolol ~ metabolized in liver (MetLv) CYP 450 S/fx: hepatotoxicity, SLE, Raynaud’s phenomenon, hepatic necrosis (rare) • Fosinopril ~ MetLv CYP450/GI S/fx: Hepatotoxicity (rare), elevated BUN,Cr, renal dysfxn/failure • V erapamil ~ MetLv CYP450:3A4 substrate/inhib. S/fx: Hepatotoxicity (rare) • aspirin ~ MetLv Salicylate CYP 450 S/fx: hepatotoxicity high dose ASA
Black Cohosh & hepatotoxic drugs • Black Cohosh has been use in German studies since the mid 1950’s for menopausal and menstrual disturbances • Eclectics have been using it in the last trimester to prepare for birth • Pharmacokinetics largely unknown • Black Cohosh has been shown to be immuno suppressive towards B-cell Fxn and at larger doses T-cell suppression has been observed • toxic doses often describe neurologic symptoms • vertigo, visual disturbance, seizures • over dose produces N/V • BLACK COHOSH<<interacts with>> CYTOCHROME P450 2D6 (CYP2D6) SUBSTRATES
Black Cohosh P450 2D6 (CYP2D6) • Some clinical research suggests that black cohosh might modestly inhibit cytochrome P450 2D6 (CYP2D6) (13536). • Some drugs metabolized by CYP2D6 include amitriptyline (Elavil), codeine, desipramine (Norpramin), flecainide (Tambocor), haloperidol (Haldol), imipramine (Tofranil), metoprolol (Lopressor, Toprol XL), ondansetron (Zofran), paroxetine (Paxil), risperidone (Risperdal), tramadol (Ultram), venlafaxine (Effexor), and others. • Use black cohosh cautiously or avoid in patients taking these drugs.
Black Cohosh & hepatotoxic drugs • There is concern that black cohosh might be linked to cases of liver failure and autoimmune hepatitis (4383,10692,11906,11909,12006,13144,14469,15160). Theoretically, taking black cohosh with hepatotoxic drugs might increase the risk of liver damage. • Advise patients against combining black cohosh with potentially hepatotoxic drugs. Some drugs that can adversely affect the liver include acetaminophen (Tylenol), amiodarone (Cordarone), carbamazepine (Tegretol), isoniazid (INH), methotrexate (Rheumatrex), methyldopa (Aldomet), and many others.
HRT • Case: AutoImmune Hepatitis in a Male-to-Female Transsexual Treated with Conjugated Estrogens. IJT 5,3, http://www.symposion.com/ijt/ijtvo05no03_03.htm • Abstract • Estrogen hormone in male-to-female transsexuals is a major component of therapy in the treatment of gender dysphoria. There are many adverse reactions to estrogen therapy that require close monitoring. We describe a case of autoimmune hepatitis that may have been exacerbated by estrogens: this is an additional adverse effect of estrogens on liver function that has not previously been reported. We recommend routine liver function tests to screen for such adverse reactions.
case of type I autoimmune hepatitis • Presented is a case of type I autoimmune hepatitis occurring in a male-to-female transsexual taking oral estrogens. The etiology of this rare liver disease is unknown. This condition occurs predominantly in young females of reproductive age (Czaja, 1996). A major clinical finding is the presence of serum autoantibodies (Czaja, 1996). Several antibodies define the type of autoimmune hepatitis. Type I is associated with positive anti-nuclear antibodies (ANA). A liver biopsy is required to confirm the diagnosis and exclude other etiologies (Czaja, 1996). Other criteria that are needed for the diagnosis include the absence of viral antibodies and other liver toxins (Johnson and MacFarlane, 1993).Treatment consists of corticosteroids alone or in combination with azothioprine (Czaja, 1996). However, treatment failure occurs in 9% of all cases and may require liver transplantation (Czaja, 1996). • Estrogens may play a role in triggering this autoimmune process: a higher prevalence of autoimmune hepatitis in pre-menopausal women has been noted by some authors (Herzog et al., 1997). This case indicates that there may be a potential adverse effect of estrogens on liver function in male-to-female transsexuals. We stress the need for careful surveillance of liver function during treatment of male-to-female transsexuals with estrogens, especially in the initial months of therapy. Liver function should be monitored every two months initially until the estrogen dose is stable; thereafter, every six months may be sufficient.
Minocycline-Related Autoimmune Hepatitis • Background Minocycline is an antibiotic commonly used in the treatment of adolescent acne. • Results Three adolescents (age, 15-16 years), while being treated with therapeutic doses of minocycline for periods of 12 to 20 months, met the 1993 International Autoimmune Hepatitis Group criteria for autoimmune hepatitis. All had a positive antinuclear antibody titer. Other features included hypergammaglobulinemia and a positive anti–smooth muscle antibody titer. Two patients underwent liver biopsy that revealed severe chronic lymphoplasmacytic inflammation, necrosis, and fibrosis. • All other causes of liver disease were excluded. One patient had resolution of symptoms with withdrawal of the drug, while 2 required immunosuppression therapy. A review of the literature yielded only 18 similar cases, none in the pediatric literature, the majority of which contained incomplete pertinent data. • Conclusions Minocycline is related to the development of autoimmune hepatitis in some adolescents. Pediatricians who use this drug for treatment of acne should be aware of this serious potential relation and stop the drug immediately when suspicion is raised. • Arch Pediatr Adolesc Med. 1998;152:1132-1136
Citation • Handbook of Liver Disease 2nd ed. Friedman,L Keeffe, E. Elsevier inc. 2004 • Principles and Practice of Phytotherapy Mills,S Bone,K 2005 Simon Mills and Kerry Bone • http://www.naturaldatabase.com/(S(mgges145e12a1o55b45q1z45))/nd/Search.aspx?cs=&s=ND&pt=100&id=857&ds=interdrug&name=Cimicifuga+(BLACK+COHOSH) • Case Report: Autoimmune HCase AutoImmune Hepatitis in a Male-to-Female Transsexual Treated with Conjugated Estrogens. IJT 5,3, http://www.symposion.com/ijt/ijtvo05no03_03.htm • Minocycline-Related Autoimmune Hepatitis Case Series and Literature Review Jonathan E. Teitelbaum, MD; Antonio R. Perez-Atayde, MD; Mark Cohen, MD; Athos Bousvaros, MD; Maureen M. Jonas, MD Arch Pediatr Adolesc Med. 1998;152:1132-1136.