Download
1 / 24
310 likes | 598 Views
Fatty Liver and Pregnancy. Shahin Merat, M.D. Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences. Case 1. 23 y/o female, GA 32 wk First pregnancy, Twin 37 kg before pregnancy Severe nausea and vomiting

E N D
Fatty Liver and Pregnancy Shahin Merat, M.D.Professor of Medicine Digestive Disease Research Institute Tehran University of Medical Sciences
Case 1 • 23 y/o female, GA 32 wk • First pregnancy, Twin • 37 kg before pregnancy • Severe nausea and vomiting • AST: 420, ALT: 350, AlkP: 382, Bil: 2.7/1.9 • Hgb: 11.2, WBC: 11,200, Plt: 107,000 • Urea: 50, creat: 2.1 • Preeclamptic • Sono: increased echogenicity
Case 2 • 34 y/o female, GA 23 • 72 kg before pregnancy • Mild nausea and vomiting • AST: 100, ALT: 130, AlkP: 340, Bil: 1.3/0.7 • Hgb: 11.2, WBC: 9,300, Plt: 249,000 • Urea: 22, creat: 0.7 • Diabetes of pregnancy • Sono: increased echogenicity
Acute fatty liver of pregnancy • Prevalence: 1 in 7000 to 1 in 20,000 deliveries • In the second half of pregnancy, usually close to term • Some patients may be diagnosed after delivery • Over half of patients have preeclampsia • Maternal mortality: 18% • Fetal mortality: 23%. • Recurrent liver disease in up to 25%.
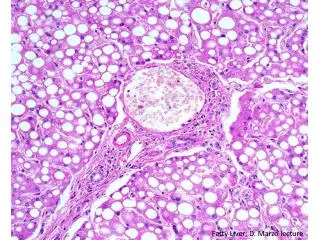
Acute fatty liver of pregnancy • Microvesicular fatty infiltration of hepatocytes without inflammation or necrosis, • perhaps due mitochondrial injury • Ultrasound detects the increased fat in liver. • More frequent in multiple pregnancy, nulliparity, male fetus, or signs of toxemia. • Maybe more frequent in underweight mothers
Symptoms • Nausea and vomiting (75%) • Abdominal pain (50%), • Anorexia • Jaundice
Lab Data • Bilirubin usually elevated • Abnormal LFT (up to 1000 IU/L) • Platelet count may be decreased, especially if with DIC • Increased WBC • PT prolongation • Hypoglycemia • Elevations in serum ammonia • ARF in up to 60% • Hyperuricemia • Overlap with HELLP • Evidence of liver failure (eg hypoglycemia, encephalopathy)
Complications • Infection • Intraabdominal bleeding • Transient central DI • Renal dysfunction • Pancreatitis
Treatment • Immediate termination • Supportive care • FFP, platelets, glucose, dialysis • Usually stabilize in 7-10 days after delivery • No liver sequel • Might repeat in next pregnancy (up to 25%)
Nonalcoholic Steatohepatitis (NASH) • Macrovesicular fat • Part of the metabolic syndrome • Three major factors • Obesity • Diabetes (or FHx of it) • Hyperlipidemia (especially TG)
NAFLD • Simple Fatty Liver • Only deposition of fat in liver • No inflammation • No fibrosis • Not believed to progress to cirrhosis • Up to 25 % of some populations! • Non-Alcoholic Steatohepatitis (NASH)
NASH - Definition • Moderate to gross macrovesicular fatty change with inflammation (lobular or portal) with or without Mallory bodies, fibrosis, or cirrhosis • Negligible alcohol consumption (<40 g/wk) • Absence of serologic evidence of infection with hepatitis B or hepatitis C
Symptoms • None!
Complications • None!
Lab Data • Elevated liver enzymes • <300 IU/L • ALT > AST • Normal AlkP, bilirubin, PT • Might have signs of impaired glucose tolerance • Hyperlipidimia • Obesity
Treatment • Treat underlying cause • Obesity • Diabetes • Hyperlipidemia • Weight loss • Exercise • Check heart
Case 1 • 23 y/o female, GA 32 wk • First pregnancy, Twin • 37 kg before pregnancy • Severe nausea and vomiting • AST: 420, ALT: 350, AlkP: 382, Bil: 2.7/1.9 • Hgb: 11.2, WBC: 11,200, Plt: 107,000 • Urea: 50, creat: 2.1 • Preeclamptic • Sono: increased echogenicity
Case 2 • 34 y/o female, GA 23 • 72 kg before pregnancy • Mild nausea and vomiting • AST: 100, ALT: 130, AlkP: 340, Bil: 1.3/0.7 • Hgb: 11.2, WBC: 9,300, Plt: 249,000 • Urea: 22, creat: 0.7 • Diabetes of pregnancy • Sono: increased echogenicity