Download
1 / 45
570 likes | 1.62k Views
Heart Disease Braunwald. Chapter 4 Physical Examination (II) --- Heart Murmur. Presenter: R4 劉嚴文. Cardiac Auscultation Heart Murmur. Characteristics of heart murmur Timing in the cardiac cycle Intensity (loudness) Frequency (pitch) --- from high to low

E N D
Heart DiseaseBraunwald Chapter 4 Physical Examination (II) --- Heart Murmur Presenter: R4 劉嚴文
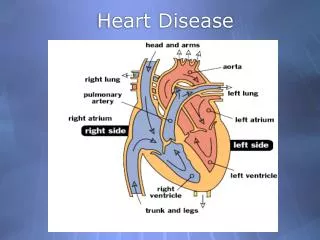
Cardiac AuscultationHeart Murmur Characteristics of heart murmur • Timing in the cardiac cycle • Intensity (loudness) • Frequency (pitch) --- from high to low • Configuration (shape) --- crescendo, decrescendo, crescendo-decrescendo (diamond-shaped), plateau (even) or variable (uneven) • Quality • Duration • Direction of radiation
Cardiac AuscultationHeart Murmur Heart murmurs broad categories • Systolic:begin with / after S1 end at / before S2 2 terms out of time • Regurgitant systolic murmur (holosystolic murmur) • Ejection systolic murmur (midsystolic murmur) • Diastolic: begin with / after S2 end at / before the subsequent S1 • Continuous: begin in systole and continue without interruption through the S2 into all / part of diastole
Midsystolic Murmurs Etiologies • Obstruction to ventricular outflow • Dilatation of the aortic root or pulmonary trunk • Accelerated flow into the normal aorta or pulmonary trunk, as during pregnancy, fever, thyrotoxicosis, or anemia • Innocent (normal) midsystolic murmurs • Some forms of MR
Aortic Valve Stenosis • Symmetrical diamond shape • High-velocity jet within the aortic root radiation of the murmur upward to the right 2nd intercostal space and the neck
Aortic Valve Stenosis • In old adults, aortic valve with sclerotic or stenotic change resulted from fibrocalcific change : • R’t 2nd ICS: impure, noisy, harsh (jet turbulence) • LV impulse: pure, musical (from periodic high-frequency vibrations of the fibrocalcific aortic cusps) ( Gallavardin dissociation--- Noisy right basal and musical apical )
Aortic Valve Stenosis D/D from high-pitch apical murmur of MR • VPC followed by pauses longer than the dominant cycle length Intensity of AS: increase Intensity of MR: unchange
Pulmonary Valve Stenosis • Location: Right side of the heart • Length and configuration: signs of severity
Still Murmur • Normal vibratory midsystolic murmur • Short, buzzing, pure and medium in frequency • Generated by low-frequency periodic vibrations of normal pulmonary leaflets or a left LV false tendon • Typically heard between LLSB and apex
Innocent Midsystolic Murmur • Location: second left intercostal space • Aortic sclerotic murmur (most common) • Exaggeration of normal ejection vibrations within the pulmonary trunk: relatively impure, best heard in the left 2nd ICS. • In patients with diminished anteroposterior chest dimension
Midsystolic Murmur from MR • Usually in ischemic heart disease associated with LV regional wall motion abnormalities. • Impaired integrity of the muscular component of the mitral apparatus • Early systolic competence of the mitral valve • Midsystolic incompetence • Late systolic decline in regurgitant flow
Holosystolic Murmurs • Left heart: MR • Right heart: TR • Between the ventricles: a restrictive VSD • Between the great arteries: Aortopulmonary connection (pulmonary vascular resistance rise to abolish the diastolic portion of the continuous murmur) A persistent high pressure / resistance systolic flow to a low pressure / resistance vascular bed
Holosystolic Murmurs Direction of radiation of MR • Jet forward and medial against the atrial septum near the origin of the aorta: murmur radiation to the left sternal edge, base and neck • Jetposterolateral with the LA: murmur radiation to the axilla, left scapula angle and the vertebral column with bone conduction from the C spine to L spine
Holosystolic Murmurs Diagnostic feature of TR • Carvallo sign --- inspiratory increasein loudness Due to increase RV volume during inspiration Stroke volume ↑ Regurgitant flow velocity ↑
Early Systolic Murmurs • Begins with S1, diminish in decrescendo and end well before S2, generally at or before midsystole • Certain types of acute severe MR, TR and VSD
Early Systolic Murmurs • A feature of TR with normal RV systolic pressure, ex. TR caused by IE • VSD • A small VSD (constrictive): a soft, pure, high-frequency, early systolic murmur localized to the mid- or lower left sternal edge • A non-constrictive VSD with elevated pulm. vascular resistance
Late Systolic Murmurs • Begin in mid- to late systole and proceed up to S2 • Prototype: Mitral valve prolapse • Response to postural maneuvers / amyl nitrite • Prompt standing after squatting / valsalva maneuver: longer and softer • Squatting / handgrip (LV volume↑): shorter and louder • An intermittent, striking systolic whoop or honk -- spontaneously or in response to maneuvers: from mitral leaflets and chordae tendineae
Heart MurmurDiastolic murmur • Early diastolic murmur AR, PR • Mid-diastolic murmur MS, TS and atrial tumors, increase flow through non-obstructive AV valve • Late diastolic murmur Austin-Flint murmur
Early Diastolic Murmurs --- AR • Left side of the heart, esp. with the diaphragm of the stethoscope • From primary valvular disease: best heard along the left sternal border in the 3rd and 4th intercostal space • From ascendingaorta dilatation: along theright sternal border • Esp. leaning forward and during a held, deep exhalation • Beginning immediately after A2, high frequency
Early Diastolic Murmurs --- AR • Chronic AR • Moderate: murmur throughout diastole • Severe: more obvious decrescendo • Radiation to the right sternal edge: aortic root dilatation, as in Marfan syndrome
Early Diastolic Murmurs --- Acute AR D/D from chronic AR Often loud, Grade 4 Quite soft, Grade 2
Early Diastolic Murmurs Graham Steell murmur (of pulmonary hypertensive pulmonary regurgitation) • Begin with loud P2 • High pulmonary pressure on the incomplete P valve High diastolic pressure gradient between the pulmonary artery and the RV High-velocity regurgitant flow High-frequency blowing murmur, throughout diastole Amplitude of the murmur: uniform throughout most of diastole
Mid-Diastolic Murmurs Mitral stenosis • Following the mitral opening snap, originating within the LV, transmission to the chest wall, maximal over the LV impulse • Left lateral decubitus position • Vigorous voluntary cough or a few sit-ups HR and mitral valve flow ↑ Murmur reinforced
Mitral stenosis • In Af, duration of the murmur is a sign of the degree of obstruction at the mitral orifice • In sinus rhythm
Mid-Diastolic Murmurs Tricuspid stenosis • D/D from MS: • Loudness of tricuspid murmur ↑with inspiration • Tricuspid murmur confined to a localized area along the left lower sternal edge
Late Diastolic Murmurs • Occur immediately before S1 • Usually originate at the mitral or tricuspid orifice because of obstruction (MS, TS) • Tricuspid stenosis: crescendo-decrescendo. Fading before S1 • Austin-Flint murmur in AR
Continuous Murmurs • PDA (loudest in left 2nd ICS) • Coronary AV fistula (loudest in lower sternal border) • Ruptured sinus of Valsalva aneurysm (loudest in right upper sternal border)
Continuous Murmurs • Arteriovenous continuous murmurs • Arterial continuous murmurs • Continuous venous murmur • Innocent cervical venous hum: the most common type of normal continuous murmur, in healthy children and healthy young adults, esp. pregnancy • Thyrotoxicosis and anemia
Approach to the Patient with a Heart Murmur • Cardiac echo is indicated as follows: • Loud murmur (>= grade 3) • Holosystolic or late systolic murmur • Systolic murmur becomes louder or longer during Valsava maneuver (susp. HOCM or MVP) • Systolic murmur with clinical findings suggesting IE, thromboembolism or syncope • Systolic murmur associated with abnormal EKG
Heart Murmur • Pericardial Rubs Triple phases midsystolic, middiastolic and late diastolic • Detected in Acute pericarditis
Dynamic AuscultationRespiration • Diastolic sounds and ejection sounds • S3, S4, opening snap • From right heart: augmented during inspiration • From left heart: diminished during inspiration • Ejection sounds intensity • Right heart, ex. PS: ↓ during inspiration • Left heart: not effected, except tetralogy of Fallot • Murmur: more pronounced on the right side murmur ( Venous return increase during inspiration ) ↑during inspiration: TS, PR (diastolic murmur), TR and Ebstein anomaly (presystolic murmur), MVP
Dynamic Auscultation • Valsalva maneuver reduced LV filling • Standing—reduce venous return • Squatting—increase venous return and systemic resistence • Lying—increase venous return • Hand grip—increase cardiac output and BP • Amyl nitritevasodilationBP drop reflex tachycardiaincrease cardiac output • Phenylephrine opposite effect of amyl nitite
Systolic Arterial Murmurs • Normal anatomical arteries with normal or increased flow • Abnormal arteries with tortuosity or luminal narrowing • Systolic and crescendo-decrescendo configuration • In old adults: atherosclerotic narrowing of a carotid, subclavian or iliofemeral artery • A rare pulmonary arterial systolic murmur: by luminal narrowing after a pulmonary embolus
Supraclavicular Systolic Murmurs • Often heard in children and aldolescents • Originate at the aortic origins of normal major branchiocephalic arteries • Crescendo-decrescendo, abrupt onset, loud and radiation below the clavicles • Murmur decrease in response to hyperextension of the shoulders
Systolic Mammary Souffle • Over the breast because of increase flow through normal arteries during late pregnancy or in lactating • Begin after S1
Mid-Diastolic Murmurs • Appreciable aortic valve incompetence or large left-to-right shunts, preceded by S3 • Short, mid-diastolic aortic valve flow murmur in complete AV block • Pulmonary valve regurgitation
Dynamic AuscultationMuller Maneuver • Close the nose and seal the mouth then forcibly inspire for 10 seconds Widen the split S2 and augment murmurs originating in the right heart
Heart MurmurSystolic murmur • Early Systolic Murmuracute MR(giant V) TR with normal RV systolic pressure • Midsystolic murmur(ejection murmur) AS, PS,VSD,ASD • Late systolic murmurMVP • Holosystolic murmur(regurgitant murmur) MR,TR(Carvallo sign selective inspiratory increase murmur),VSD