Download
1 / 46
470 likes | 866 Views
Twins & Higher Multiple Gestations. Dr. Ahmed Al Harbi Obstetrics/Gynecology Consultant. Definition . MULTIPLE PREGANCIES consists of two or more fetuses . TWINS make up the vast majority (97-98%) of multiple gestations.

E N D
Twins & Higher Multiple Gestations Dr. Ahmed Al Harbi Obstetrics/Gynecology Consultant
MULTIPLE PREGANCIES consists of two or more fetuses . TWINS make up the vast majority (97-98%) of multiple gestations. Pregnancies with three or more fetuses are referred to as ‘higher multiples’.
In the UK, twins currently account for approximately 1.5% of all pregnancies. Higher multiples occur in 1 in 2,500 pregnancies.
Risk factors for multiple gestation include: Reproduction Techniques (Both ovulation and in-vitro fertilization or IVF) Increasing maternal age High parity Black Race Maternal family history
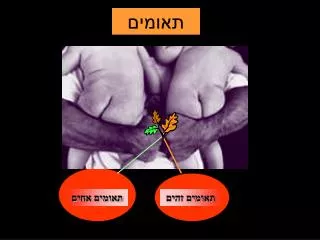
Classification of multiple pregnancy Number of fetuses: twins, quadruplets, etc. Number of fertilized eggs: zygosity Number of placentas: chorionicity Non identical or fraternal twins are dizygotic, having resulted from the fertilization of two separate eggs. Two functionally separate placentas (dichorionic)
They always have separate amniotic cavities (diamniotic) and the two cavities. The fetuses can be either same-sex or different-sex-pairings. Identical twins are monozygotic- they arise from fertilization of a single egg and are always same-sex pairings. Monochorionic twins may occasionally share a single sac (monoamniotic).
Not all dichorionic pregnancies are dizygotic. All monochorionic pregnancies are monozygotic.
Dizygotic twins may arise spontaneously from the release of two eggs at ovulation The tendency to release more than one egg can be familial or racial in origin and increases with maternal age. Monozygotic twins arise from a single fertilized ovum that splits into two identical structures.
The type of monozygotic twin depends on how long after conception the split occurs. When the splits occurs within 3 days of conception, two placentas and two amniotic cavities result, giving rise to a dichorionic diamniotic (DCDA) pregnancy. When splitting occurs between days 4 and 8, only the chorion has differentiated and a monochorionic diamniotic (MCDA) pregnancy results.
Later splitting after the amnion has differentiated leads to both twins developing in a single amniotic cavity, a monochorionic monoamniotic (MCMA) pregnancy. If splitting is delayed beyond day 12, the embryonic disc has also formed, and conjoined or ‘Siamese’ twins will result. It is not influenced by race, family history or parity.
MATERNAL All the physiological changes of pregnancy (increased cardiac output, volume expansion, relative haemodilution, diaphragmic splinting, weight gain, lordosis, etc.) are exagerated in multiple gestations.
FETAL Monochorionic placentas have the unique ability to develop vascular connections between the two fetal circulations. These anastomoses carry the potential for complications.
Miscarriage & Severe Preterm Delivery General Therefore about half of all twins deliver preterm. As most babies born from 32 weeks onwards do very well, births at 34 or 35 weeks carry little clinical significance. In contrast, almost all babies born at 23 weeks or less die, with rates of mortality and handicap steadily falling between 24 and 31 weeks.
Perinatal Mortality In Twins General The overall perinatal mortality rate for twins is around six times higher than for singletons. The biggest contributor to this high rate is complications related to preterm birth. Dichorionic / Monochorionic Differences As preterm delivery is most common in monochorionic twins, their perinatal mortality secondary to this is twice as high as in dischorionic twins.
Death of one fetus in a twin pregnancy General After the 1st trimester, the intrauterine death of one fetus in a twin pregnancy may be associated with a poor outcome for the remaining co-twin. Dichorionic / Monochorionic Differences Acute hypotensive episodes, secondary to placental vascular anastomoses between the two fetuses, result in haemodynamic volume shifts from the live to the dead fetus. Death or handicap of the co-twin occurs in up to 25% of cases.
Intrauterine Growth Restriction General The risk of poor growth is higher in each individual twin alone and substantially raised in the pregnancy. Dichorionic / Monochorionic Differences The chance of poor fetal growth for monochorionic twins is almost double that for dichorionic twins.
Fetal abnormalities General Compared to singletons, twins the risk of the birth of a baby with an anomaly. Dichorionic / Monochorionic Differences Each fetus of a dichorionic twin pregnancy has a risk of structural anomalies, such as spina bifida. Anencephaly is a good example of a lethal abnormality that can threaten the survival of the normal twin.
Complications Unique To Monochorionic Twinning Twin-to-twin transfusion syndrome (TTTS). The donor fetus suffers from both hypovolaema due to blood loss and hypoxia due to placental insufficiency, and may become growth-restricted and oliguric. This fetus develops oligohydramnios. The recipient fetus becomes hypervolaemic, leading to polyuria and polyhydramnios.
There is a risk of myocardial damage and high output cardiac failure. Severe disease may become apparent at 18-24 weeks of pregnancy. The mother often complains of a sudden increase in abdominal girth associated with extreme discomfort.
Differential Diagnosis • The differential diagnosis of a multiple gestation includes all the other causes of a ‘large for dates’ uterus: polyhydramnios, uterine fibroids, urinary retention and ovarian masses .
AntenatalManagement • Routine antenatal care for all women involves screening for hypertension and gestational diabetes. • These conditions occur more frequently in twin pregnancies and there is also a higher risk of other problems (such as antepartumhaemorrhage and thromboembolic disease).
Determination of chorionicity Screening for fetal abnormalities The optimal method of screening twins is by ultrasound. The measurement of nuchal translucency at 12 weeks gestation allows each fetus to have an individualized assessment of risk. Both amniocentesis and chorion villus sampling (CVS)
Monitoring fetal growth & well-being Monitoring for fetal growth and well-being in twins is principally by ultrasound scan. Each assessment should include fetal measurement, fetal activity, fetal lies and amniotic fluid volumes. In monochorionic twins, features of TTTS should be sought, including discordances between fetal size, fetal activity, bladder volumes, amniotic fluid volumes and cardiac size. Doppler assessment of the fetal circulations and cardiotocography (CTG).
Threatened preterm labour Antenatal strategies in those identified as at high risk may include screening for bacterial vaginosis (treatment may eliminate a co-factor for spontaneous preterm labour), screening for group B Streptococcus (GBS; intrapartum antibiotics reduce neonatal infection), maternal steroid therapy to enhance fetal lung maturation.
Once preterm is diagnosed, neonatal unit staff must be promptly involved. The use of tocolytic drugs in this situation, particularly the beta-agonists, carries risks of serious maternal morbidity. Multiple pregnancy support groups
Preparation A twin CTG machine should be used for fetal monitoring and a portable ultrasound machine should be available during delivery. A standard oxytocin solution for augmentation should be prepared, run through an intravenous giving-set and clearly labelled ‘for augmentation’, for use for delivery of the second twin, if required.
A second high-dose oxytocin infusion should also be available for the management of postpartum haemorrhage. It is essential that two neonatal resuscitation trolleys, two obstretricians and two paediatricians are available and that the special care baby unit and anaesthetist are informed well in advance of the delivery.
Analgesia during labour Epidural analgesia is recommended. Fetal well-being in labour Fetal heart rate monitoring should be continuous throughout labour, ideally using a speciallized twin monitor. An abnormal fetal heart rate pattern in twin I may be assessed using fetal scalp sampling, as for a singleton pregnancy. However, a non-reassuring pattern in twin 2 will usually necessitate delivery by Caesarean section. The condition of twin 1, as acute complications such as cord prolapse and placental separation are well recognized.
Vaginal delivery of vertex-vertex Delivery of the first twin is undertaken in the usual manner and thereafter the majority of second twins will be delivered within 15 minutes. After the delivery of the first twin, abdominal palpitation should be performed to assess the lie of the second twin. It is helpful to use ultrasound for confirmation, which is also useful for checking the fetal heart rate. If the lie is longitudinal with a cephalic presentation, one should wait until the head is descending and then perform amniotomy with a contraction.
If contractions do not ensue within 5-10 minutes after delivery of the first twin, an oxytocin infusion should be started. If an assisted delivery becomes necessary, the vacuum extractor has a number of advantages. Delivery of vertex-non-vertex Non-vertex first twin When twin 1 presentation as a breech, clinicians usually recommend delivery by elective Caesarean section. Other factors include dwindling experience of breech delivery and the rarely seen phenomenon of ‘locked twins’.
Preterm twins Even in low-birth-weight twin gestations, the method of delivery in relation to fetal presentation will have little or no effect on neonatal mortality and subsequent neonatal development outcome. No significant differences in perinatal outcome exist when comparing breech-extracted second twins to those delivered by Caesarean section.
Requirements for twin delivery Large delivery room Operating theatre and staff ready Anaesthetist present Senior obstetrician present At least two midwives present Twin resuscitaires Ventous/forceps to hand Blood grouped and saved Intravenous access Neonatologists present Pre-mixed oxytocin infusion ready