Download
1 / 47
470 likes | 716 Views
Electronic Discharge Prescriptions at Princess of Wales Hospital. Rowena Duffield. Electronic Transfer of Care ( eTOC ). First ward in May 2007 Now on over 440 beds Provides GP with a detailed list of medicines on day of discharge Pre-existing medicines

E N D
Electronic Discharge Prescriptions at Princess of Wales Hospital Rowena Duffield
Electronic Transfer of Care (eTOC) • First ward in May 2007 • Now on over 440 beds • Provides GP with a detailed list of medicines on day of discharge • Pre-existing medicines • Dose changes to pre-existing medicines • New medicines and reason for starting • Stopped medicines and reason for stopping
Electronic Transfer of Care • Junior doctor fills in the • initial review • test results • diagnosis • procedures • medication • management plan • follow up arrangements • Pharmacist verifies and signs off medication • Consultant or senior registrar signs off clinical summary
Transfer to GP • On the day of discharge the GP gets: diagnosis, medication list, management plan, follow up arrangements • Once the whole form is signed off the GP gets the complete summary
Comments from GPs • “Useful and timely” • “Much clearer which medicines are pre-existing, new or stopped” • “Much easier to map information onto patient medication record” • “Has reduced errors due to poor transcription and illegibility”
In summary • We have an electronic discharge prescription and discharge summary sent directly to the GP • We send the medicines list on the day of discharge for 97% of patients
Investigation into incidence, types and causes of prescribing errors on handwritten and electronic discharge prescriptions. MSc Dissertation
Background to project • Prescribing errors are a risk to patient safety • Electronic prescriptions have been shown to increase patient safety • Electronic discharge prescriptions implemented in Princess Of Wales • Investigate prescribing error rate on paper (TTH) and electronic (eTOC) discharge prescriptions
Objectives of project • To determine the proportion of prescribing interventions on TTHs and eTOCs • To categorise the types of prescribing interventions on TTHs and eTOCs • To compare the severity of errors made on a sample of TTHs and eTOCs • To identify prescribers’ ideas or reasons to the causes of errors on eTOCs and potential solutions.
Methods • Retrospective collection of completed TTHs and eTOCs • Sample of TTH and eTOC errors graded for severity by nurses/doctors/pharmacists • 15 prescribers interviewed, doctors that made most errors and all four nurse prescribers
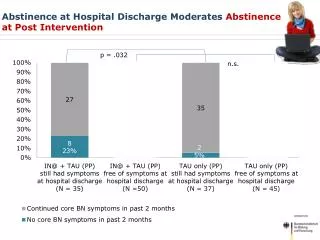
Results from TTHs and eTOCs • 336 TTHs analysed • 2028 items in total • 23% items had intervention • 71% TTHs had intervention • 12% items had error • 44% TTHs had ≥1 error • 342 eTOCs analysed ↔ • 3491 items in total ↑ • 22% items had intervention ↔ • 76% eTOCs had intervention ↔ • 16% item had error ↑ • 60% eTOCs had ≥1 error ↑ No difference in rates of interventions Odds of eTOC having an error were 1.95 times higher than a TTH
Comparing like-for-like errors only • The extra types of error on eTOCs contributed ~35% of all errors • Comparing like-for-like errors only results in significantly more errors on TTHs than eTOCs • Odds of item having error on TTH is now 1.62 times higher than on eTOC Overall intervention rate now significantly higher on TTHs than eTOCs
Association between types of error and types of prescription
Majority of prescribing at discharge was by more junior doctors(data only available for eTOCs)
Comparison of prescribing showed a trend of increasing error rate with number of years experience as a doctor
Other comments about errors • There were significantly more errors on Medicine and Elderly Care prescriptions than General Surgery and Trauma and Orthopaedics • Significantly more errors on TTHs for respiratory medicines
Researchers’ estimations of severity of errors showed significant differences
The severity of errors made by F1s and NPs tended to be of lower severity than from doctors with greater number of years’ experience
Severity Judging • Sample of eTOC and TTH errors • Judged by nurses, doctors and pharmacists • Range of specialties (including 2 GPs) • Visual analogue scale 0-10cm • Mean scores calculated for each error • Researchers’ estimation confirmed in 87.5% cases Mean scores for eTOC errors were lower than TTH errors
Interviews with Prescribers • 15 interviews • Range of grades and specialties • Audio-taped and transcribed verbatim • Transcripts analysed looking for causes of errors
Causes of Prescribing Errors • Documentation -EPC • Many errors blamed on poor documentation • Prescribers couldn’t find information in the notes • Decisions made without entries in notes • Changes made to chart with no explanation • But prescribers didn’t always look back through all the notes because it was too time-consuming
Causes of Prescribing Errors • Legibility in notes and on charts -EPC • “Sometimes it is difficult because you have to work out what the hell the drug is, there is poor handwriting on drug charts” (NP) • Time Pressure – Error producing condition • “I think the reason why errors occur is due to the time on the ward. I don’t have time to do them properly” (CT1)
Causes of Prescribing Errors • Distractions on the ward • “when you’re on the ward, you’re doing a few things at a time, and you’ve got to sit down and do this properly, and sometimes that’s not always possible, you’re called to do different things” (F1)
Causes of Prescribing Errors • Unfamiliar with eTOC -EPC • “Those of us who do it more regularly just get on with it, those who do it infrequently aren’t going to be familiar with it” (CT2) • Unfamiliar with medication • “a major error on the Epo, it’s on as one three times a week, and it should have been twice a week. Epo isn’t a medicine I’m familiar with, and normally when I prescribe things I know in my head whether it’s clearly wrong and it wouldn’t have been an error I’d pick up on when inputting it onto the computer” (F2)
Causes of Prescribing Errors • Unfamiliar with patient • Being absent during ward round • Prescription for patient under a different team • Cover prescriber on nurse-led rehab ward • “It is more difficult to do it if you don’t know the patient, because normally we are not seeing the patient and then you have to go to rehab ward and do an eTOC for the patient” (F2)
Causes of Prescribing Errors • More than one person involved in eTOC -EPC • “This is an example of where the nurse practitioners look after the patients throughout their journey in the rehab ward including the eTOC and they put in all these details for the patients. I am aware of them, but I haven’t checked every detail on it which is why these errors have occurred” (Registrar)
Causes of Prescribing Errors • Length of stay of patient - EPC • Errors more likely to occur when chart rewritten • “when I do the eTOCs I only use current charts, that is something to be aware of” (F1) • Other causes: • “pressure on the doctors” (F2) • “an oversight” (CT2) • “not taking due care and attention” (NP)
Knowledge of Errors • Awareness of mistakes • “With things like inhalers I was pretty sure I was making mistakes with those” (F2) • “If I would have known I wouldn’t have done it! (laughs)” (F2) • Change of practice • “You only learn from knowing about your mistakes, so now that I’m more aware, I think I’ll be more careful next time” (CT1)
Knowledge of Errors • Feedback • “You are never going to able to improve if you don’t know what you’re doing wrong, you’re just going to keep doing it” (F2) • Consequences • “GPs have to know from this exactly what happened during the admission, and if it’s not precise the GP doesn’t know what’s going on, and that can be highly detrimental” (CT2)
Prescription PreferenceMore preferred TTH to eTOCbut many felt eTOCis superior communication Advantages of TTHs • Speed of handwriting over typing • Takes less time out of their day • Satisfies nursing requests faster • Only needs to be list of medicines Disadvantages of TTHs • Legibility problems due to poor handwriting • Less detail about medicines given to GP • Limited transfer of information onto carbon copies if prescribers pressed lightly
Advantages of eTOCs • Short codes for dosing instructions • Instant access to a perfectly legible copy of prescription in a clinic or if patient re-admitted • Benefits of improved information transfer to the GP outweighed the downsides of the eTOC Disadvantages of eTOCs • The requirement to enter clinical details such as diagnosis • One prescriber thought that the increased demand for information may lead to more errors on eTOCs • Inconvenience of eTOC lay with computers not the form itself or level of detail required • E.g. slow computers, password problems or not enough computers
Types of Errors • Name of drug • “I know it’s not good to make errors, but creams and eye drops is stuff that I consider to be a bit ‘over-the-counter’…” (CT2) • Form of drug • “If it’s not written on the chart, I just guess!” (CT1) • “I know there are lots of different types of inhalers and it’s beyond me sometimes” (F1)
Types of Errors • Date of initiation • “Sometimes you just put ‘prescribed before admission’ for everything because it’s the easy option” (CT2) • Omission • “Umm… not sure why I’ve missed them, perhaps the patient had a second chart?!” (F1)
Other comments • Computer related problems • Speed of computers and availability on wards • “I think once you’ve got the hang of doing it, you can do it quite quickly - computer speed dependent” (F1) • Pharmacist annotations • “Yeah because otherwise we wouldn’t have a clue, cos often, even if you look in the clerking notes, the doctor could have missed stuff off, or we’re not sure whether it has just been started. The annotations from the pharmacist I rely on a lot” (F1)
Other comments • Differences between grades of prescriber • “Nurse prescribers may be better, especially with inhalers, cos they open the locker and give it to the patient, whereas we never clap eyes on it. They may be better at trade names as well” (F1) • “I think you probably get worse as you get more experienced, cos I think registrars will be far less familiar with eTOC” (F2)
Other comments • Suggestions to improve eTOC • “I’m not sure anything can be done, it’s just more time consuming, but these things do need to be communicated to the GP” (F2) • Positives about eTOC • “I often use them if we’ve got someone coming into A&E and I haven’t got a clue about their history, I open [the eTOC], they are really useful to know what meds they have been on in the past” (F2) • “We don’t have discharge summaries anymore because they took an eternity to do, this is a combined process, it’s much easier” (CT2)
Suggestions to reduce errors • Attend training asap and ask for help • Start eTOC early in admission • Allow time to do eTOC without rushing • Write clearly on charts and in notes • Fully document all decisions in notes/on chart • Justify prescribing choices in notes • Use original medication history • Extra care with long admission/many changes
Suggestions to reduce errors • Be mindful of distractions on the ward • Don’t allow undue interruptions • Be conscious of unfamiliar medicines • Be aware anyone can make mistakes • Responsibility lies with final prescriber • Ask for feedback from pharmacist
In Summary… • Significantly more errors on eTOCs when looking at all possible error types • Omission most common type of error • When looking at like-for-like error types only, eTOCs had significantly fewer overall interventions and errors • F1s and NPs had lowest error rates
In Summary… • Significantly more minor and fewer major errors on eTOCs • F1s and NPs made more minor and fewer major errors than doctors with more years’ experience • Mean severity scores for eTOC errors were consistently lower than for TTHs
In Summary… • Interviews highlighted many causes of errors • Time pressure, poor documentation, distractions on the ward • Being unfamiliar with the medicine, patient, or eTOC system increased chances of error
Since the project finished • Met with pharmacists to discuss what we could do to help • Decided to fully endorse all types of inhalers • Ensure endorsements transcribed onto rewritten charts • Met with Consultants to share results and discuss how we use this data to improve prescribing
Since the project finished • Consultants interested in findings and surprised by some interview quotes • Felt junior doctors had to take more responsibility for providing good communication to GPs • Gave me permission to present to junior doctors • Junior doctors felt only extra time and less pressure would reduce error rates