Download
1 / 56
560 likes | 676 Views
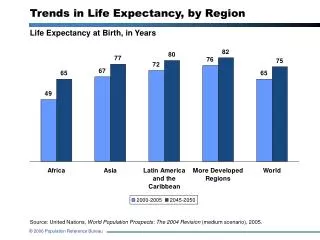
Life expectancy trends. Portugal. Scotland. Trends in male life expectancy: Scotland. Richest 20%. Poorest 20%. World Health Organization (1997 and 2003). www.heartstats.org. Smoking prevalence - Males. Males. Smoking prevalence - Females. Females. Income deprivation - Liverpool.

E N D
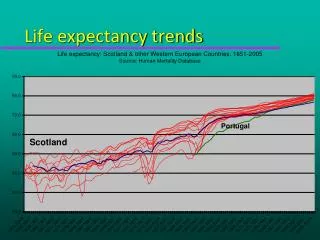
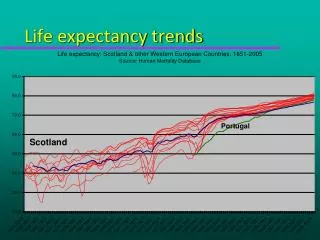
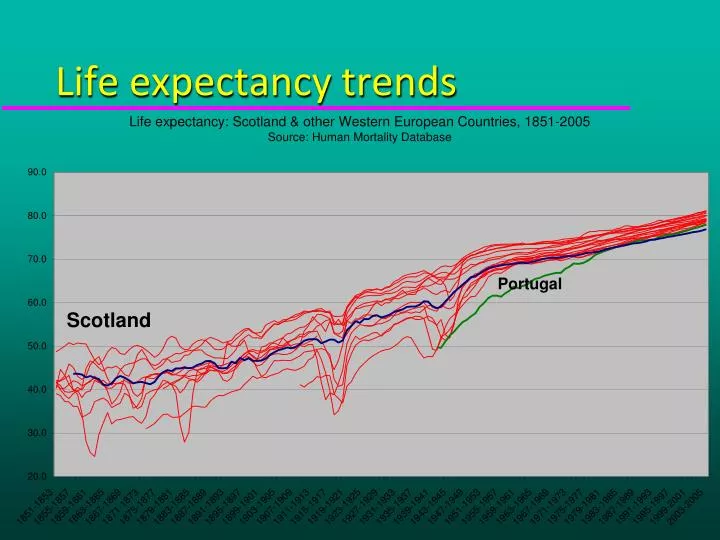
Life expectancy trends Portugal Scotland
Trends in male life expectancy: Scotland Richest 20% Poorest 20%
World Health Organization (1997 and 2003) www.heartstats.org
Smoking prevalence - Females Females
Standardised mortality rates by cause, all ages: Glasgow relative to Liverpool & Manchester Source: Walsh D, Bendel N., Jones R, Hanlon P. It’s not ‘just deprivation’: why do equally deprived UK cities experience different health outcomes? Public Health, 2010
Alvin Toffler – Future Shock 1970 • “To survive, to avert what we have termed future shock, the individual must become infinitely more adaptable and capable than ever before. We must search out totally new ways to anchor ourselves, for all the old roots - religion, nation, community, family, or profession - are now shaking under the hurricane impact of the accelerative thrust.
Sense of coherence.... “.....expresses the extent to which one has a feeling of confidence that the stimuli deriving from one's internal and external environments in the course of living are structured, predictable and explicable, that one has the internal resources to meet the demands posed by these stimuli and, finally, that these demands are seen as challenges, worthy of investment and engagement."
....the social and physical environment must be: Comprehensible Manageable Meaningful ......or the individual would experience chronic stress For the creation of health....
“A child who lacks a sense of coherence interprets all the events around him as noise not as information. This he finds very stressful” Antonovsky
STRESS AND GRADE OF EMPLOYMENT: MEN Salivary Cortisol Time of Day Steptoeet al. 2003, Psychosomatic Medicine, 65, 461-470
Environmental determinants of inflammatory status CRP(median) mg/dl affluent deprived
Inflammation in plaques cytokines MMP Lumen Inflammatory Cells Degraded matrix SMC apoptosis Cap Core Inflammatory cells MMPs, IL-6, IL-15, IL-18, CRP Thin Fibrous Cap Unstable
CRP and cumulative risk of type 2 diabetes % diabetic Q5: > 4.18 mg/l 5 4 3 2 1 Q1 : <0.66 mg/l 0 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Years in study Freeman et al. Diabetes 2002,51;1596
Adipocyte programminginsulin resistance, inflammation and ALP skeletal muscle Insulin resistance triglyceride Atherogenic Lipoprotein Phenotype NEFAs Low HDL small LDL Adipose stores liver IL-6/IL-6sR CRP SAA Pro-inflammatory state TNF-a/ TNF-a sR-I
Attachment theory Ainsworth Deep emotional connection that infant develops with primary caregiver Reflects an “internal working model”expressing the infant’s expectations of parental behaviour in meaningful situations Basis for development of later relationships Increasingly recognised as determinant of later emotional, cognitive and social outcomes
Adverse childhood events study • Physical/sexual/emotional abuse • Neglect (physical/emotional) • Domestic substance abuse • Domestic violence • Parental mental illness • Parental criminality
Adverse childhood events risk of alcoholism Hillis et al 2011
Adverse childhood eventsrisk of perpetrating violenceBoys experiencing physical abuse Duke et al 2010
The Dunedin cohort 1000 children recruited in late 1972/3 At age 3, “at risk” children identified on the basis of chaotic circumstances, emotional behaviour, negativity and poor attentiveness As adults, those “at risk” were more likely to : be unemployed have criminal convictions (especially for violence) been pregnant as a teenager have a substance abuse problem exhibit signs of insulin resistance and metabolic syndrome
Creating wellbeing Generalised resistance resources Family Intelligence Work Material Identity Cultural stability Optimism Stable set of answers Sense of coherence Seeing the world as: Structured Predictable Feeling that it is: Manageable Meaningful Wanting to engage Events Stress Resolution Wellbeing
Do social conditions determine the incidence of disease? • For centuries they have and they still do in the developing world • Plague, leprosy, polio, diphtheria, typhoid, tuberculosis • BUT in the developed countries • It is mainly our physiological responseto social conditions which largely determines our risk of chronic ill health
Focuses on problems, needs and deficiencies in a community such as deprivation, illness and health damaging behaviours. It designs services to fill the gaps and fix the problems. As a result, communities can feel disempowered. People become passive recipients of services rather than active agents in their own lives Health Deficits approach
Social connectedness • 148 studies comprising 308,849 participants, high levels of social integration conferred a 50% increased likelihood of survival. • Complex patterns of social integration conferred a 90% increase in survival. • Simple indicators such as living alone versus living with others conferred a survival benefit of only 19%.
A health asset is any factor or resource which enhances the ability of individuals, communities and populations to maintain their health and sustain wellbeing. The assets can operate…as protective and promoting factors to buffer against life’s stresses Health Assets Morgan 2009
Alienation and Frankenstein • "I came across people, other beings which I could see were almost like myself. Or so I thought at first when I approached them, though, I found that they did not consider me as one of their own kind. As soon as they saw me, their faces became twisted with fear. They shouted at me and threw things and ran away from me, just as my own maker had done. So this is what I learned about myself - that I was a disgusting creature. Even though I had given them no cause, all men hated me."
The pathology of poverty 24th European Congress of Pathology Prague 11th September 2012