Download
1 / 45
450 likes | 618 Views
Staging and Management of Genital Prolapse. Dr. V.P.Paily MD; FRCOG Professor Jubilee Mission Medical College, Thrissur, Kerala. Consultant, Mother Hosp and Raji Nursing Home , Thrissur, Kerala. Prolapse. Very common problem.

E N D
Dr. V.P.Paily MD; FRCOG Professor Jubilee Mission Medical College, Thrissur, Kerala. Consultant, Mother Hosp and Raji Nursing Home , Thrissur, Kerala
Prolapse • Very common problem. • Confusion regarding assessing degree / stage
Conventional Staging • Cervix is the main point.
Conventional staging • Difference between British and American System.
Baden Walker Halfway System
Prolapse quantification • Pelvic organ prolapse quantification(POP-Q) • Recommended by ICS, society of Gyn.Surgeons &Amer. Urogyn. Surgeons
Pelvic organ prolapse • Quantification • POP Q
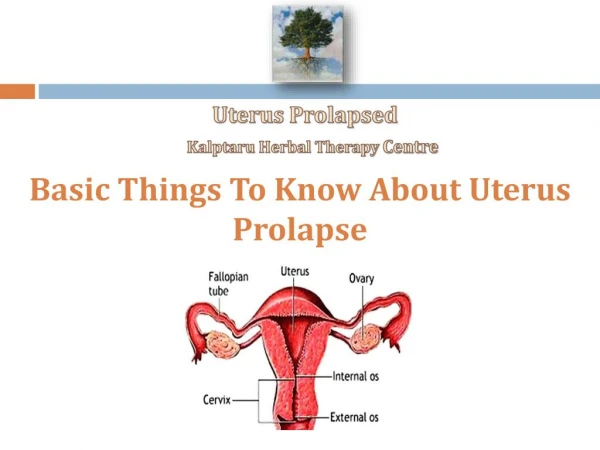
Quantification • Vault, Cx or Posterior fornix • Anterior & Posterior walls • Introitus • Perineal body • Length of vagina
Quantification • Anterior (a) -- Point A & B • Posterior (p) -- Point A & B • Point C -- Lips of Cervix • Point D -- Post.fornix
Quantification • Length of vagina • Diameter of introitus • Perineal body
POP-Q Drawbacks • Appears complicated • Doesn’t include lateral prolapse.
Comprehensive pattern required incorporating defects at various levels & compartments
Look for defects At 3 levels Upper Middle Lower
Look for defects At two compartments • Anterior • Posterior
Compartmental approach Level 1 • Descent of cervix • Descent of vault • Enterocele
Compartmental Approach Level 2 • Anterior segment – cystocele • Posterior segment – rectocele • Lateral detachment
Compartmental Approach Level 2 • High rectocele can extend up to post fornix and has to be differentiated from enterocele.
Compartmental Approach Level 2 • Midline defects are due to tear or weakness of fascial envelope – pubo vesico cervical fascia and rectovaginal fascia ( Denonvilliers).
Compartmental Approach Level 3 • Anteriorly – Urethrocele • Posteriorly – Detached perineal body
Compartmental Approach Level 3 • Detached Perineal body • Reattach to recto vaginal fascia
Practical approach to Level 3 defects • Common complaint Sound of air being sucked in
Compartmental Approach Lateral detachment • Reattach to Arcus Tendineus • Fascia pelvis or Arcus Tendineus • Fascia Rectovaginalis
Compartmental Approach Anterior Lateral detachment • Richardson’ s operation • Transvaginal • Transabdominal • Endoscopic
Compartmental Approach Posterior Lateral detachment • Reattach to Arcus tendineus fascia rectovaginalis
Symptomatology Record symptoms related to • Anatomical descent • Urinary function • Sexual function • Reproductive need • GI symptoms • Air suction
Management • Restore anatomy by correcting the defect.
Mesh for Repair • Concept borrowed from Hernia repair • Special mesh being developed. (Gyne mesh) • We have tried prolene mesh.
Conclusions • Detailed record of defects • Detailed record of symptoms • Individualised surgery