Download
1 / 50
500 likes | 648 Views
Emerging results from the AEDI: implications for Australia's children. Associate Professor Sharon Goldfeld Paediatrician and Research Fellow Centre for Community Child Health, Royal Children's Hospital Murdoch Childrens Research Institute sharon.goldfeld@rch.org.au.

E N D
Emerging results from the AEDI: implications for Australia's children Associate Professor Sharon Goldfeld Paediatrician and Research Fellow Centre for Community Child Health, Royal Children's Hospital Murdoch Childrens Research Institute sharon.goldfeld@rch.org.au
“A society that is good to children is one with the smallest possible inequalities for children, with the vast majority of them having the same opportunities from birth for health, education, inclusion and participation.” (Stanley, Richardson & Prior, 2005)
Overview • Why early childhood matters • Why literacy matters • Why data matter • Health and developmental inequalities in Australia: the results of the AEDI • Community as a potential platform for change
Building strong foundations Getting the foundations right is important – healthy brain development is a prerequisite for future health and wellbeing.
Key experiences shaping health & developmentEarly language and cognitive stimulation
Developmental health opportunity Ideal child-development trajectory Opportunity Current practice At-risk child-development trajectorywithout intervention Age
Return on investment in the early years Reference: Cunha et. al., 2006.
Impact of adversity early in life Hackman D, Farah M, Meaney M. Socio economic status and the brain: mechanistic insights from human and animal research. Neuroscience. Vol11 2010; 651-659
69% of NT Indigenous children score belownational minimum standard
Targeting low-ses students v. targeting low performing students Source: Masters (2009) using PISA data
Creating sustainable policy: Recognition of the problem Identification of the solution through policy Evidence based policy Data Children on the policy agenda Political imperative Kingdon J. Agendas, Alternatives and Public Policies. 2nd ed. New York: Harper Collins College Publishers, 1995
Health and developmental inequalities in Australia: the results of the AEDI
The AEDI is a relative population measure of how young children are developing in different Australian communities.
The AEDI looks at how groups of children are developing and reports back on how groups of children are developing. It gathers information on each child…
What is the aim of the AEDI? To measure the health and development of populations of young children to assist communities and governments to plan and assess the effectiveness of their efforts in supporting young children and their families.
National implementation: • National data collection from 1 May to 31 July 2009 • Data collected by teachers through a secure web based data entry system • Schools provided with funding of 1 hour for teacher training and 30 minutes per completed checklist • Data analysed and reported based on where children live • AEDI were re-run in small communities in 2010.
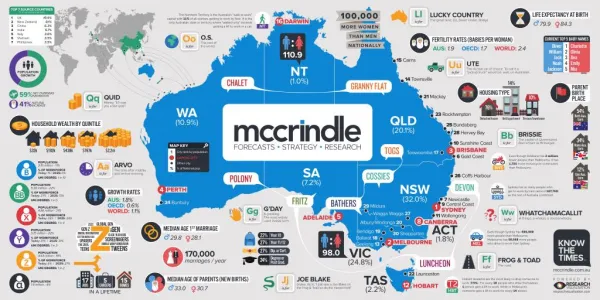
2009 snapshot of Australia’s children: Northern Territory: 3,255 Queensland: 55,449 WA: 27,579 NSW: 87,168 SA: 16,208 ACT: 4,432 Victoria: 61,196 Tasmania: 5,916 Total = 261,203 children (97.5% of estimated population)
National Numbers Data collected on 261, 203 children (97.5%). 15,528 teachers from 7,423 schools (95.6% of all schools) participated. Teacher feedback (86.4% of all teachers, n=13,815): 90.1% found AEDI easy to complete 63.9% thought AEDI will be beneficial to their work 74.8% felt the AEDI will assist their community to better understand the health and development of children in their area
Key Findings Percentage of children developmentally vulnerable (DV) across Australia by jurisdiction
Australian Indigenous children and SEIFA: Percentage developmental vulnerability Green = Vulnerable on one or more domains Yellow = No vulnerability
Australian Indigenous children and SEIFA: Number developmentally vulnerable Green = Vulnerable on one or more domains Yellow = No vulnerability